




Cancer
AI could help improve early detection of interval breast cancer

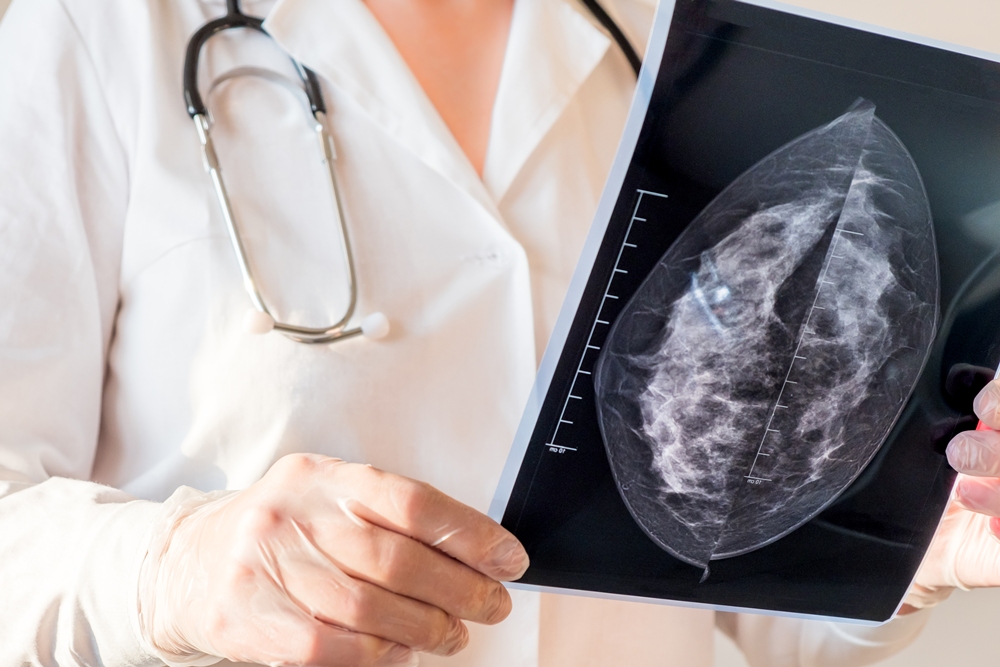
A new study suggests that AI could help detect interval breast cancer — those that develop between routine screenings — before they become more advanced and harder to treat. This could potentially lead to better screening practices, earlier treatment and improved patient outcomes.
The study, led by investigators at the UCLA Health Jonsson Comprehensive Cancer Center and published in the Journal of the National Cancer Institute, found that AI was able to identify “mammographically-visible” types of interval cancers earlier by flagging them at the time of screening.
These include tumours that are visible on mammograms but not detected by radiologists, or have very subtle signs on mammography that are easy to miss because the signs were faint or arguably below the level of detection by the human eye.
Researchers estimate that incorporating AI into screening could help reduce the number of interval breast cancers by 30 per cent.
“This finding is important because these interval cancer types could be caught earlier when the cancer is easier to treat,” said Dr. Tiffany Yu, assistant professor of Radiology at the David Geffen School of Medicine at UCLA and first author of the study.
“For patients, catching cancer early can make all the difference. It can lead to less aggressive treatment and improve the chances of a better outcome.”

While similar research has been conducted in Europe, this study is among the first to explore the use of AI to detect interval breast cancers in the United States. Researchers point out that there are key differences between the US and European screening practices.
In the US, most mammograms are performed using digital breast tomosynthesis (DBT), often called 3D mammography, and patients are typically screened every year. In contrast, European programmes usually use digital mammography (DM), often called 2D mammography, and screen patients every two to three years.
The retrospective study analysed data from nearly 185,000 past mammograms from 2010 to 2019 that included both DM and DBT. From the data, the team looked at 148 cases where a woman was diagnosed with interval breast cancer.
Radiologists then reviewed these cases to determine why the cancer wasn’t spotted earlier. The new study adapted a European classification system to categorize the interval cancers. They include: Missed reading error, minimal signs–actionable, minimal signs–non–actionable, true interval cancer, occult (which is truly invisible on mammogram), and missed due to a technical error.
Researchers then applied a commercially available AI software called Transpara to the initial screening mammograms performed before the cancer diagnosis to determine if it could detect subtle signs of cancer that were missed by radiologists during initial screenings, or at least flag them as suspicious. The tool scored each mammogram from 1 to 10 for cancer risk. A score of 8 or higher was considered flagged as potentially concerning.
The team found that the AI flagged 76 per cent of the mammograms that had been originally read as normal but were later linked to an interval breast cancer. It flagged 90 per cent of missed reading error cases where the cancer had been visible on the mammogram but missed or misinterpreted by the radiologist.
It caught 89 per cent of minimal-signs-actionable cancers that showed very subtle signs and could reasonably have been acted upon, as well as 72 per cent of those with minimal-signs-non-actionable that were likely too subtle to prompt action.
For cancers that were occult or completely invisible on the mammogram, the AI flagged 69 per cent of cases.
It was somewhat less effective at identifying true interval cancers, those that were not present at the time of screening but developed later, flagging 50 per cent.
“While we had some exciting results, we also uncovered a lot of AI inaccuracy and issues that need to be further explored in real-world settings,” said Dr. Hannah Milch, assistant professor of Radiology at the David Geffen School of Medicine and senior author of the study.
“For example, despite being invisible on mammography, the AI tool still flagged 69 per cent of the screening mammograms that had occult cancers. However, when we looked at the specific areas on the images that the AI marked as suspicious, the AI did not do as good of a job and only marked the actual cancer 22 per cent of the time.”
Larger prospective studies are needed to understand how radiologists would use AI in practice and address key questions, such as how to handle cases where AI flags areas as suspicious that aren’t visible to the human eye, especially when the AI isn’t always accurate in pinpointing the exact location of cancer.
“While AI isn’t perfect and shouldn’t be used on its own, these findings support the idea that AI could help shift interval breast cancers toward mostly true interval cancers,” Yu added.
“It shows potential to serve as a valuable second set of eyes, especially for the types of cancers that are the hardest to catch early. This is about giving radiologists better tools and giving patients the best chance at catching cancer early, which could lead to more lives saved.”












Changes in AI mammogram scores may help predict breast cancer years before diagnosis, research involving more than 54,000 women suggests.
Scores rose steadily among women who later developed the disease but remained broadly stable among those who did not.
The increase could be detected up to six years before diagnosis and became much steeper during the final two years.

Researchers led by Professor Constance Lehman, of Harvard Medical School and healthcare technology company Clairity, analysed screening mammograms taken between 2009 and 2019.
They used a validated, open-source deep learning model to calculate five-year breast cancer risk scores from the images alone.
Deep learning is a form of artificial intelligence trained to recognise complex patterns in large amounts of data.
The model examined the whole mammogram rather than relying on a limited, predetermined feature such as breast density.
Models of this kind have performed better than traditional risk models and breast density alone when estimating a woman’s five-year breast cancer risk.
The study initially included 239,703 consecutive two-dimensional screening mammograms from 89,882 patients across six imaging sites spanning urban tertiary, community-based and rural settings.
All were standard bilateral full-field digital mammography examinations, taken with or without digital breast tomosynthesis.
Digital breast tomosynthesis uses multiple low-dose X-ray images to create a three-dimensional view of the breast.
After exclusions, the final analysis involved 54,014 women with a median age of 61 and a total of 158,807 mammograms.
Each woman contributed one index examination and up to six previous annual mammograms. Women had a median of three scans each.
For women who developed cancer, the index examination was their final screening mammogram within the year before diagnosis. For the cancer-free group, it was their final mammogram during the five-year study period.
The model did not use demographic information, clinical records or historical imaging data when calculating each score.
Of the women included, 817, or one per cent, were diagnosed with breast cancer within 365 days of their index examination.
This included 451 women, or 55 per cent, with invasive breast cancer and 118, or 14 per cent, with ductal carcinoma in situ, known as DCIS.
DCIS occurs when abnormal cells are found inside a milk duct but have not spread into the surrounding breast tissue.
The cancer type was unknown for the remaining 248 patients, representing 30 per cent of the cancer group.
A total of 682 cancers, or 83 per cent, were detected through screening, while 135, or 17 per cent, were interval cancers diagnosed between routine mammograms.
The other 53,197 women were not diagnosed with breast cancer during follow-up and formed the cancer-free comparison group.
Professor Lehman said: “We observed clinically relevant differences in risk trajectories between women who did and did not develop cancer. The increase in scores among cancer patients was detectable as early as six years prior to diagnosis and became more pronounced over time.”
Among women later diagnosed with the disease, the median score rose from 2.1 five to six years before diagnosis to 6.6 at the index examination.
Scores among cancer-free women remained stable, with median values ranging from 1.8 to 2.2 throughout the study.
The rise among women who developed cancer was steepest during the two years before their index examination.
Professor Lehman said: “These findings demonstrate signals, invisible to the human eye, in the image alone can predict future risk. This is exciting, because 85 per cent of women diagnosed with breast cancer do not have a significant family history of breast cancer or known genetic mutations.”
Most breast cancers are considered sporadic, meaning they are not driven by inherited genetic changes or a family history of the disease.
Traditional risk models have a limited ability to distinguish between women who will and will not develop breast cancer when used across large screening populations.
Researchers said tracking how scores change over time could provide more information than calculating risk at a single appointment.
Professor Lehman said: “AI-derived risk scores can identify patients who are otherwise predisposed to the disease, and our findings demonstrate that image-based AI risk scores evolve over time and that changes in those scores may provide additional information about future breast cancer risk.”
The patterns remained consistent when women were grouped by age and breast density.
Breast density describes the amount of fibrous and glandular tissue visible on a mammogram. Dense tissue can make cancers harder to detect and is also associated with an increased risk of the disease.
Researchers said image-based scores could support personalised screening and risk-reduction strategies without relying on self-reported or inconsistent clinical information.
Professor Lehman said: “These trends remained robust across subgroups defined by age and breast density, further supporting the generalisability of our findings. This is particularly relevant given persistent disparities in screening performance across patient populations. A dynamic biomarker approach grounded in the imaging data could mitigate some of these disparities by enabling risk-based personalisation that does not rely on self-reported or inconsistent clinical data.”
A biomarker is a measurable sign that can indicate a person’s health, disease risk or response to treatment.
Changing scores could eventually help clinicians identify women who may benefit from additional imaging or measures intended to reduce their risk.
Professor Lehman said: “With the power of AI, computer vision, and the ability to extract predictive data, we are able to apply the power of imaging to risk assessment and preventing disease from developing. Having a dynamic risk score opens up a whole new domain of more effective preventive therapies for breast cancer, similar to how we screen for and treat patients with high cholesterol and hypertension.”
AI image-based risk scores are included in the 2026 National Comprehensive Cancer Network guidelines.
The guidelines recommend that, from the age of 35, women with an elevated five-year risk score of more than 1.7 per cent consider breast MRI alongside annual mammography.
An AI image-based model approved by the US Food and Drug Administration is already being used to calculate five-year breast cancer risk at selected US healthcare institutions.

WID-easy, the only non-invasive triage test for endometrial cancer in routine use in a European public health system, has been cited in Germany’s highest-tier clinical guidance; a marker that non-invasive detection is reaching clinical maturity.
The vaginal-swab test designed to spare women unnecessary invasive procedures has been referenced in the updated German S3 Guideline on Endometrial Cancer, its maker Sola Diagnostics has announced.
The Austria-based women’s-health diagnostics company behind the WID-easy Test, said the test now features in the recommendations-supporting background text of the guideline’s latest version (v4.0, May 2026; AWMF 032-034OL), in Section 4.3.
The S3 designation is the highest evidence- and consensus-based tier in the German clinical guideline system, broadly comparable in standing to NICE guidance in the UK, and is widely drawn on in clinical practice, reimbursement and liability assessments.
In Section 4.3, the guideline cites four peer-reviewed validation studies of the WID-easy Test and credits it with a sensitivity of more than 95 per cent and a negative predictive value of at least 99.7 per cent.
It describes a fall in invasive workup from 19 to two dilatation-and-curettage (D&C) procedures per cancer detected when compared with transvaginal ultrasound alone, assuming a realistic 3.4 per cent cancer prevalence in women with postmenopausal bleeding, and states that the test has the potential to improve the diagnostic workup of women with peri- and post-menopausal bleeding by cutting the rate of invasive procedures.
A growing burden, an imperfect standard
Endometrial cancer is the most common gynaecological cancer in high-income countries, and its incidence is rising, driven by ageing populations and increasing obesity, making it one of the fastest-growing cancer burdens in women’s health.
A number of groups are now developing non-invasive tests for earlier detection. The current standard, transvaginal ultrasound, is an imperfect triage tool: it misses serous carcinomas and performs especially poorly in black women, a group with disproportionately high endometrial-cancer mortality.
WID-easy has been validated prospectively across multiple cohorts, including a dedicated cohort of black women in Ghana (Ken-Amoah et al., 2025).
Adopted in routine care
WID-easy is the only endometrial-cancer triage test in Europe with real-world adoption in a public health system. It is UKCA-marked and in use across NHS pilot sites in England and Scotland, and is delivered through commercial laboratory partners across the DACH region of Austria, Germany and Switzerland. Its UK pivotal study, EASY-CARE, is funded by a competitively awarded NIHR i4i grant.
The postmenopausal bleeding pathway has been singled out for change across three UK Government strategy documents published in 2026 — the National Cancer Plan for England (DHSC), the renewed Women’s Health Strategy for England (DHSC) and the National HealthTech Access Programme (NICE).
The NICE initiative names speeding up access to better tools for detecting endometrial cancer in women with unexplained bleeding as one of only four priority areas.
WID-easy is the only non-invasive endometrial-cancer triage test that is UKCA-marked and commercially available for NHS use today, with no competing molecular test yet on the market.
“Seeing WID-easy referenced in a guideline of this standing confirms that the science behind non-invasive endometrial cancer detection has reached clinical maturity,” said Prof Martin Widschwendter, founder and member of the scientific advisory board at Sola Diagnostics.
“Our goal has always been to spare women unnecessary invasive procedures without missing the cancers that matter — and to do so equitably, across all populations.”
The WID-easy Test detects and triages endometrial cancer from a vaginal swab using DNA methylation. It is built on the WID-qEC biomarker, exclusively licensed from University College London Business and complemented by Sola’s own patent portfolio. The same methylation platform underpins a pipeline of further tests in cervical, ovarian and breast cancer.

The HPV vaccine has cut the risk of dying from cervical cancer before age 30 to almost zero among those vaccinated at 12 or 13, research suggests.
The first study of its kind found that deaths have fallen sharply since school-age girls began being offered the jab in 2008, with around 200 lives saved in England so far.
Between 2020 and 2024, no cervical cancer deaths were recorded among women aged 20 to 24, the first time this had happened over a five-year period.

Without vaccination, around 23 deaths would have been expected.
Professor Peter Sasieni, lead researcher at Queen Mary University of London, said: “It’s incredible to think that a single jab can almost eliminate a particular type of cancer.”
Around 3,300 people are diagnosed with cervical cancer each year in the UK, making it the 14th most common cancer among women.
Human papillomavirus, or HPV, is thought to cause 99 per cent of cervical cancer cases. The virus is spread through close skin-to-skin contact.
Most HPV infections clear up without causing problems, but some can cause abnormal cell changes that may lead to cancer years later.
The study’s authors expect deaths from cervical cancer to continue falling as more people receive the jab and vaccinated generations grow older.
Cancer Research UK, which funded the research, called the findings an “incredible milestone” but warned that vaccination rates in England remained below recommended levels.
Michelle Mitchell, chief executive of Cancer Research UK, said: “We know the HPV vaccine is extremely effective at stopping cervical cancer before it starts and for the first time these findings show it is saving lives.”
Professor Sasieni, who specialises in cancer epidemiology at Queen Mary University of London, described the reduction in deaths since the vaccine was introduced as the “tip of the iceberg”.
Cancer epidemiology examines patterns of cancer and how the disease affects different groups of people.
He said: “As vaccinated generations grow older, we’ll see many more lives saved from cervical cancer.
“New research shows just how vital it is to keep HPV vaccination levels high so more people are protected.”
The UK government has pledged to eliminate cervical cancer as a public health problem by 2040.
However, the latest figures show vaccination rates have fallen below recommended levels.
UK Health Security Agency data shows that 76 per cent of girls in England were vaccinated by the age of 15 in 2024-25, well below the 90 per cent level the World Health Organization says is needed to eliminate cervical cancer.
Mitchell said: “It’s essential that the UK Government and health systems urgently address this with targeted action to reach communities where uptake is the lowest.”











 News2 weeks ago
News2 weeks agoOvum secures US$4m in seed funding

 Entrepreneur2 weeks ago
Entrepreneur2 weeks agoXella launches AI-powered precision health platform

 Insight2 weeks ago
Insight2 weeks agoMost IVF add-ons not backed by reliable evidence, research finds

 Fertility2 weeks ago
Fertility2 weeks agoImmunotherapy may temporarily restore fertility in premature menopause

 News2 weeks ago
News2 weeks agoEU committee warns of women’s health ‘blind spot’

 News2 weeks ago
News2 weeks agoDon’t miss HTW’s upcoming deep dive into health AI
 Insight2 weeks ago
Insight2 weeks agoChanges in AI mammogram risk scores help predict future breast cancer

 News4 days ago
News4 days agoBreast cancer biosensor and low-cost ultrasound startups win women’s health AI competition
1 Comment