




Opinion
Defunding equity: The Big Beautiful Bill and the broader crisis in women’s health innovation

By Melissa Wallace, CEO & Founding Partner, Fierce Foundry
Imagine if half the population were quietly being cut off from funding, resources, and opportunity. No protests, no headlines—just policies dressed up as reform.
For women, and for those building what little infrastructure exists to support us, this isn’t fiction. It’s policy in action.
Funding is quietly frozen. Grant programmes disappear overnight. Tax policy gets “revised.” And somehow, always, it’s the programmes that support women’s health, economic mobility, and safety that end up on the chopping block.
It’s important to share what this really means but also identify ways we can push back.
A Coordinated Attack Disguised as ‘Efficiency’
Earlier this year, the Department of Justice’s Office on Violence Against Women pulled all open funding opportunities from its site with zero warning.
At the time of writing, the OVW’s homepage showed no active grants available, an eerie confirmation of the freeze.
This isn’t theoretical. These are grants that keep crisis hotlines open. That put lawyers in courtrooms to help women file restraining orders. That ensures shelters can literally keep their lights on.
Then the only federal program focused solely on family planning, Title X, froze $65 million in funding. Again, just look at their homepage.
Providers forced out because of a revived gag rule. Entire counties with no reproductive health access. Proving again, this is not just about budgets.
And more importantly, there’s the NIH.
What was and should always be the gold standard of American medical research, the NIH is now being slowly gutted from the inside out, facing capped indirect costs, grant freezes, and the loss of over 1,000 employees.
Research on maternal mortality, reproductive health, and gender-based health disparities is stalled or abandoned at a time when women’s health outcomes in the U.S. are already in crisis.
Grad programs are pausing admissions. Institutions are rescinding job offers.
It’s crazy to think that if your research centers on women, you’re no longer a priority.
Female Founders Are Feeling It Too
At our Venture Studio, Fierce Foundry, we co-build FemTech companies led by women, so we see firsthand how policy disruptions are stifling innovation.
Leslie Feinzaig at the Female Founders Alliance recently surveyed hundreds of women entrepreneurs. The numbers are brutal:
- 47 per cent say today’s economy is hurting their business, not because their ideas are weak, but because they’re navigating a toxic mix of cautious buyers, inflation, and frozen grant programmes.
- 46 per cent say the political climate is actively harming them, with NIH, DoD, and EPA listed as the most disrupted funding sources.
- Even those who raised money in early 2025: 48 per cent still report negative fallout because the ground keeps shifting beneath them.
We’re not witnessing random cuts. We’re watching a playbook unfold.
When the only thing more unstable than the market is the government meant to support it, you create an environment where risk tolerance drops to zero, and guess who pays the price in a system already biased against women?
Enter H.R.1, the Velvet Hammer
Otherwise known as the ironically named “One Big Beautiful Bill Act”, Congress recently passed H.R.1, a 600+ page legislative mic drop wrapped in “anti-corruption” branding.
In reality, it’s another blow to the nonprofit and startup sectors, especially the ones working in women’s health, climate, education, and equity.
This new law:
- Complicates how nonprofits advocate, effectively muting mission-driven organisations with compliance red tape
- Disincentivises charitable giving by eliminating the universal charitable deduction
- Weakens the Johnson Amendment, opening the door to political manipulation inside nonprofits
Layer this over the already shaky landscape created by the administration’s targeted funding cuts, and you get what looks a lot like a strategic dismantling of the nonprofit sector, death by a thousand policy decisions.
This Isn’t Just Budgeting—It’s a Turning Point
It’s tempting to see these cuts as routine cost-saving measures.
But the patterns tell another story, and it demands our attention.
When funding consistently disappears from domestic violence shelters, reproductive healthcare, scientific research, and community-led nonprofits, we have to ask:
What kind of future are we shaping?
When accountability measures are framed as anti-corruption but silence the very voices meant to advocate for equity, it’s not just government that shrinks, it’s trust, access, and progress.
And those bearing the brunt? Women. Especially women of colour. Especially those building solutions in sectors already under-resourced. Especially those who believed our public systems were meant to include them.
But here’s the opportunity: recognising these patterns allows us to shift course. To build systems that are transparent, equitable, and truly serve the public good.
We have a chance to reimagine not just restore what support for women can and should look like.
So What Now?
This is our moment of reckoning and of responsibility.
If you’re outraged, good. But outrage without action changes nothing.
Call your representatives. Ask them where they stand on funding for the NIH, Title X, and nonprofit protections.
Demand they reverse the cuts that are crippling women’s health and innovation.
Join organisations like the National Council of Nonprofits, League of Women Voters, and Protect Our Care that are tracking these shifts and mobilising action.
Subscribe to policy trackers like G2G, and stay engaged on federal rule changes
affecting women’s health innovation.
Support women-led startups and nonprofits, especially the ones filling gaps left by the government.
And if you have a platform, use it.
Encourage your company to support advocacy coalitions or match donations to affected nonprofits.
The future of FemTech depends on more than great ideas and breakthrough science, it depends on a system willing to invest in women’s health, protect equity-driven founders, and fund the research that saves lives.
When the scaffolding holding up women’s progress collapses, it’s not just women who fall; it’s all of us.
Research proves that when women are economically empowered, communities thrive.
Countries with greater gender equality have stronger economies, healthier families, and more resilient democracies.
When we support women, we don’t just protect half the population; we invest in the whole.
References
- “Trump DOJ freezes domestic violence grants, leaving shelters and legal services scrambling”
Politico, March 1, 2025
https://www.politico.com/news/2025/03/01/funding-freeze-domestic-violence-00206807
- “Trump administration halts Title X family planning funding in 23 states”
TIME Magazine, April 2025
https://time.com/7276543/title-x-funding-freeze-threatens-states
- “Planned Parenthood Faces Steep Financial Losses Amid Trump Budget Cuts”
Wall Street Journal, May 2025
https://www.wsj.com/politics/policy/planned-parenthood-abortion-trump-supreme-court-a0c54920
- “Second Presidency of Donald Trump” (NIH Grant Freeze and Layoffs) Wikipedia summary based on multiple government sources, 2025 https://en.wikipedia.org/wiki/Second_presidency_of_Donald_Trump
- “I Am Seeing My Community of Researchers Decimated” The New Yorker, February 2025
https://www.newyorker.com/news/deep-state-diaries/i-am-seeing-my-community-of-researchers-decimated
- “Trump Administration Slashes Millions in NIH Funding for Maternal Health, HIV, and Other Research”
Protect Our Care, 2025
https://www.protectourcare.org/its-a-bloodbath-trump-administration-slashes-millions-in-nih-funding
- “2025 Female Founder Sentiment Survey”
Female Founders Alliance / Leslie Feinzaig, Q2 2025
(Direct data provided – no public link currently available)
- “New Tax Law Threatens Nonprofits’ Ability to Serve Communities” National Council of Nonprofits, April 2025
- “Congress Passes Major Tax Package—Nonprofits Directly Impacted” National Council of Nonprofits, April 2025
- “4 Key Elements of H.R.1”
League of Women Voters, March 2025
https://www.lwv.org/blog/4-key-elements-hr1
11.“Trump’s War on the Nonprofit Sector”
The Guardian, April 2025
https://www.theguardian.com/us-news/2025/apr/10/trump-administration-authoritarian












By Jane Lewis, chief operating officer, chief financial officer and women’s health lead, ABHI
For years, the conversation around women’s health has rightly focused on recognition.
Recognition that women wait longer for diagnosis. Recognition that symptoms are too often dismissed or normalised. Recognition that healthcare systems have historically been designed around male biology, leaving gaps in research, evidence and care.
That recognition matters. But awareness alone will not improve outcomes.
The challenge facing women’s health today is no longer simply identifying the problem. It is acting on the solutions already available.
At ABHI’s Women’s Health Summit earlier this year, leaders from across healthcare, government, academia and industry came together to discuss the future of women’s health.
One message emerged repeatedly throughout the day: we do not have an innovation problem.
Across medical devices, diagnostics, digital health and genomics, there are already technologies capable of transforming outcomes for women.
From self-sampling approaches for cervical screening and non-invasive diagnostics to AI-enabled tools and advanced imaging, innovation is happening. The question is whether healthcare systems can adopt it quickly enough.
Too often, promising technologies become trapped in pilot programmes, fragmented procurement processes or lengthy implementation pathways. Evidence generation, commissioning and adoption are frequently treated as separate challenges rather than part of a single journey.
The consequence is that innovations capable of improving quality of life and reducing pressure on health services take years to reach the women who could benefit from them.
This matters because women’s health extends far beyond reproductive health.
Historically, many discussions have centred on fertility, pregnancy and gynaecological conditions. These remain critically important, but they represent only part of the picture.
Women experience cardiovascular disease differently to men. They are disproportionately affected by autoimmune conditions. They face distinct health challenges throughout their lives, from adolescence to healthy ageing.

Jane Lewis
Yet healthcare systems often continue to approach these issues in isolation.
A woman does not experience her health in separate compartments. Pregnancy, cardiovascular risk, menopause, mental health and musculoskeletal conditions are interconnected.
Healthcare systems need to reflect that reality through more integrated, life-course approaches to care.
There has never been a better opportunity to do so.
Across the NHS, the shift towards prevention, community-based care and digital transformation aligns closely with the needs of women’s health.
Women’s Health Hubs are already demonstrating the benefits of bringing services together around the needs of women rather than organisational boundaries. Digital technologies are helping to identify risk earlier and support more personalised care.
Innovation can help deliver all three of the NHS’s major transformation ambitions: moving from treatment to prevention, from hospital to community, and from analogue to digital care.
But innovation alone is not enough.
Closing the women’s health gap also requires us to address longstanding gaps in research and evidence.
Women remain underrepresented in many areas of clinical research, and sex-disaggregated analysis is not always applied consistently. The result is that clinical pathways and treatment decisions are often based on evidence that does not fully reflect female physiology.
Better data, stronger research participation and greater focus on female-specific and female-predominant conditions will be essential.
There is also a compelling economic case for action.
Women’s health is often framed as an equality issue, and equality remains central. But poor health affects workforce participation, productivity and economic growth.
Improving outcomes for women benefits not only patients, but employers, healthcare systems and wider society.
Yet despite this, women’s health innovation continues to attract only a fraction of the investment directed towards other areas of healthcare.
That is beginning to change.
Across the UK and internationally, momentum is building. Governments, investors, researchers and innovators increasingly recognise that women’s health is both a societal necessity and an economic opportunity.
The conversation has moved on significantly in recent years. Topics that were once overlooked are now firmly on the policy agenda.
The next challenge is ensuring that awareness translates into action.
The technologies exist. The evidence is growing. The policy direction is increasingly clear.
ABHI is increasingly taking this agenda beyond national boundaries. Through our engagement with international industry associations, policymakers and healthcare leaders, we are working to ensure that women’s health is recognised as both a health and economic priority.
We are helping to shape discussions on innovation, regulation, investment and adoption, while sharing lessons from the UK with partners around the world.
Whether addressing the gender health gap, improving access to diagnostics or accelerating the uptake of new technologies, international collaboration will be essential.
The challenge now is not recognising the need for change, but delivering it.
Women have waited long enough for acknowledgement of the problem. They should not have to wait any longer for the benefits of the solutions that already exist.
ABHI is the UK’s leading industry association for HealthTech. Its members, ranging from multinationals to small and medium-sized enterprises (SMEs), develop and supply technologies spanning everything from syringes and wound dressings to surgical robots, diagnostics, and digitally enabled healthcare solutions. ABHI’s 400 member companies represent approximately 80% of the UK HealthTech sector by value.

By Dr Fran Conti-Ramsden, clinician at Guy’s and St Thomas’ NHS Foundation Trust, academic at King’s College London, and chief medical officer of MEGI Health.
A woman gives birth. A few days later she goes home, often with a bag of medication for her blood pressure, and then, very often, very little structured follow-up for her heart (cardiovascular) health.
In my clinical work, and through our collaboration with Action on Pre-eclampsia, I see and hear about this postnatal cliff edge again and again, and it still shocks me.
We invest a lot of medical care and attention whilst a woman or birthing individual is pregnant, then, at the very moment emerging evidence suggests we have a window of opportunity to modify long-term health, the support falls away.
That cliff edge is a symptom of a deeper issue: we have come to treat “women’s health” as a synonym for reproductive health. Pregnancy, periods and fertility, important as they are, have crowded out everything else.
Yet the conditions that do most to shorten and limit women’s lives are not reproductive at all.
Cardiovascular disease is the leading cause of death in women worldwide, and it is still too readily thought of as a man’s problem.
Heart disease in women is more likely to be missed and under-treated, in part because for decades women were under-represented in the research that built our knowledge.
Pregnancy makes this vivid.
Conditions such as pre-eclampsia are not only risks to be managed for nine months; they are early warnings about a woman’s future, markers that she is more likely to develop heart disease and high blood pressure in the years to come.
We have the knowledge to act on that. What we mostly do instead is discharge her and look away.
This is exactly the kind of problem better tools should help us solve: spotting risk earlier, supporting women and their clinicians through the vulnerable postnatal window, and providing continuity where the system currently provides a drop due to lack of capacity.
Artificial intelligence and digital health have real potential here; in risk prediction, in monitoring blood pressure at home, and in helping stretched clinicians know who needs attention and when.
And yet this is not where most of the energy is going.
It is far easier to build, fund and scale an app that tracks a cycle than a tool that changes the trajectory of a woman’s heart.
So, innovation clusters at the lighter, lower-risk end of innovation, while the conditions that actually kill and disable women, and moments like the postnatal cliff, stay under-served.
Closing the women’s health gap could add at least a trillion dollars to the global economy each year, the World Economic Forum estimates, but the bigger prize is women living longer, healthier lives.
None of this means technology is a cure in itself. It is a tool, and a tool built carelessly can do harm.
Because women have been under-represented in medical data, systems trained on that data can quietly carry the same blind spots forward, deepening inequalities rather than closing them.
Responsible innovation, with clinical-grade evidence, privacy and equity designed in from the start, and tools built around real clinical pathways rather than bolted on afterwards, is not a brake on progress.
It is the only version of progress worth having.
I am optimistic, because a serious community is forming around exactly these questions and the appetite to get it right is real.
It is why, at MEGI, we are bringing clinicians, researchers, founders, regulators and investors together for our AI × Women’s Health summit on 25 June.
If we keep our focus on the conditions that matter most to women’s lives, and build the tools to meet them responsibly, the postnatal cliff edge could become something else entirely: the moment the system finally catches her and delivers preventative healthcare.
AI × Women’s Health: Innovation, Challenges and Opportunities summit is taking place on Thursday 25 June 2026 at the London Institute for Healthcare Engineering. The event is free and is fully booked and operating a waiting list. Join the waiting list here.
About Dr Fran Conti-Ramsden
Dr Fran Conti-Ramsden is a UK Obstetrics and Gynaecology registrar and Chadburn Clinical Lecturer at KCL passionate about transforming women’s health through technology and innovation.
Combining NHS clinical experience with an MRC-funded PhD, recent NHS Clinical AI fellowship and commercial role as Chief Medical Officer at Megi health, she works at the intersection of clinical medicine, data science, technology and AI.
Her current programme of research focuses on the intersection of healthcare and technology; leveraging advances such as smartphone based vital signs capture and large language models to drive forward scalable innovation in maternal cardiovascular care.
She has published over 20 peer-reviewed manuscripts (See gScholar, h-index 12), including award-winning work recognized by Hypertension Journal.
She was awarded an AI visionary award in 2025 by Health Innovation KSS was the recipient of the 2024 International Society for the Study of Hypertension in Pregnancy Zuspan prize.


By Women As One
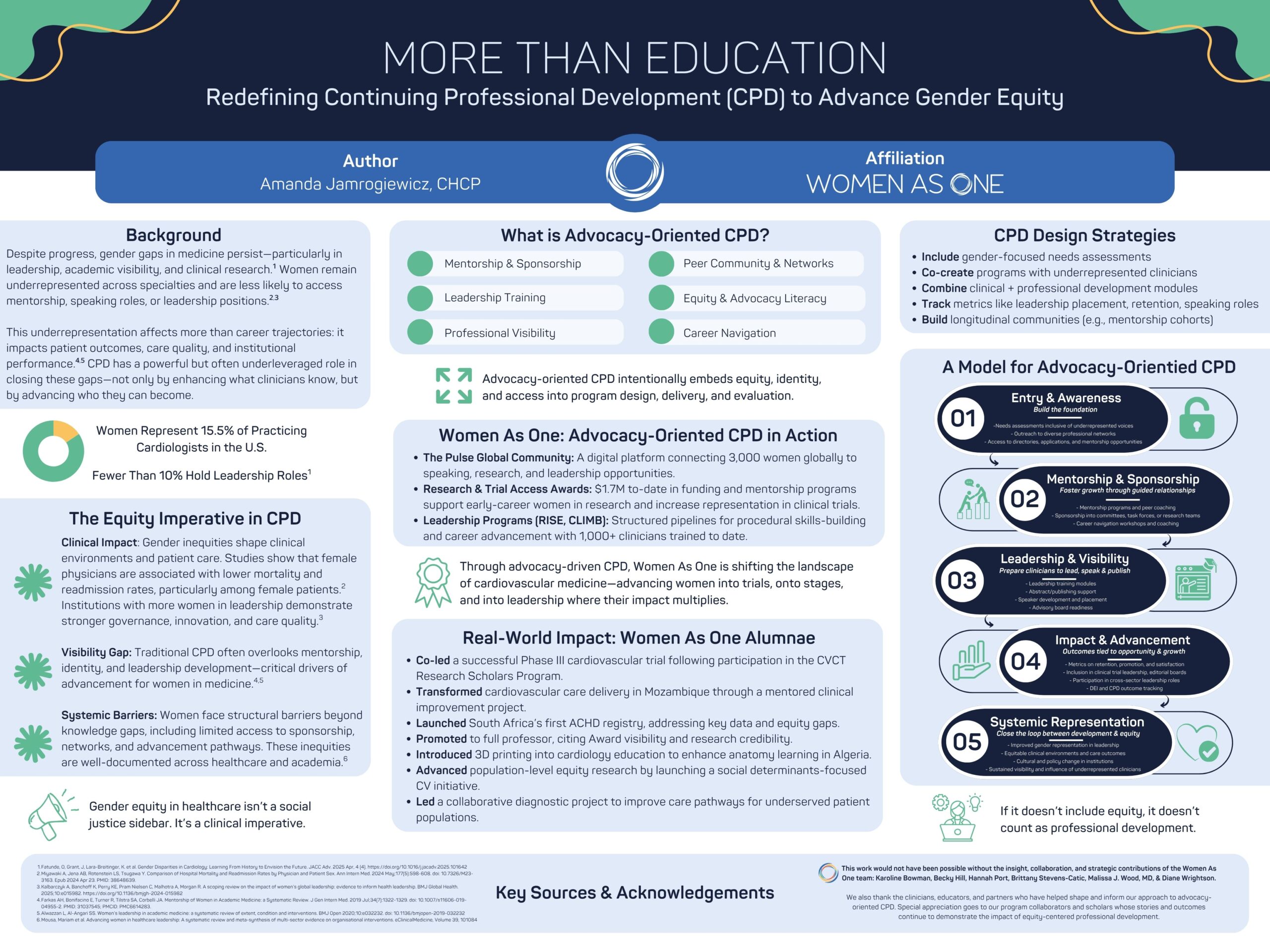
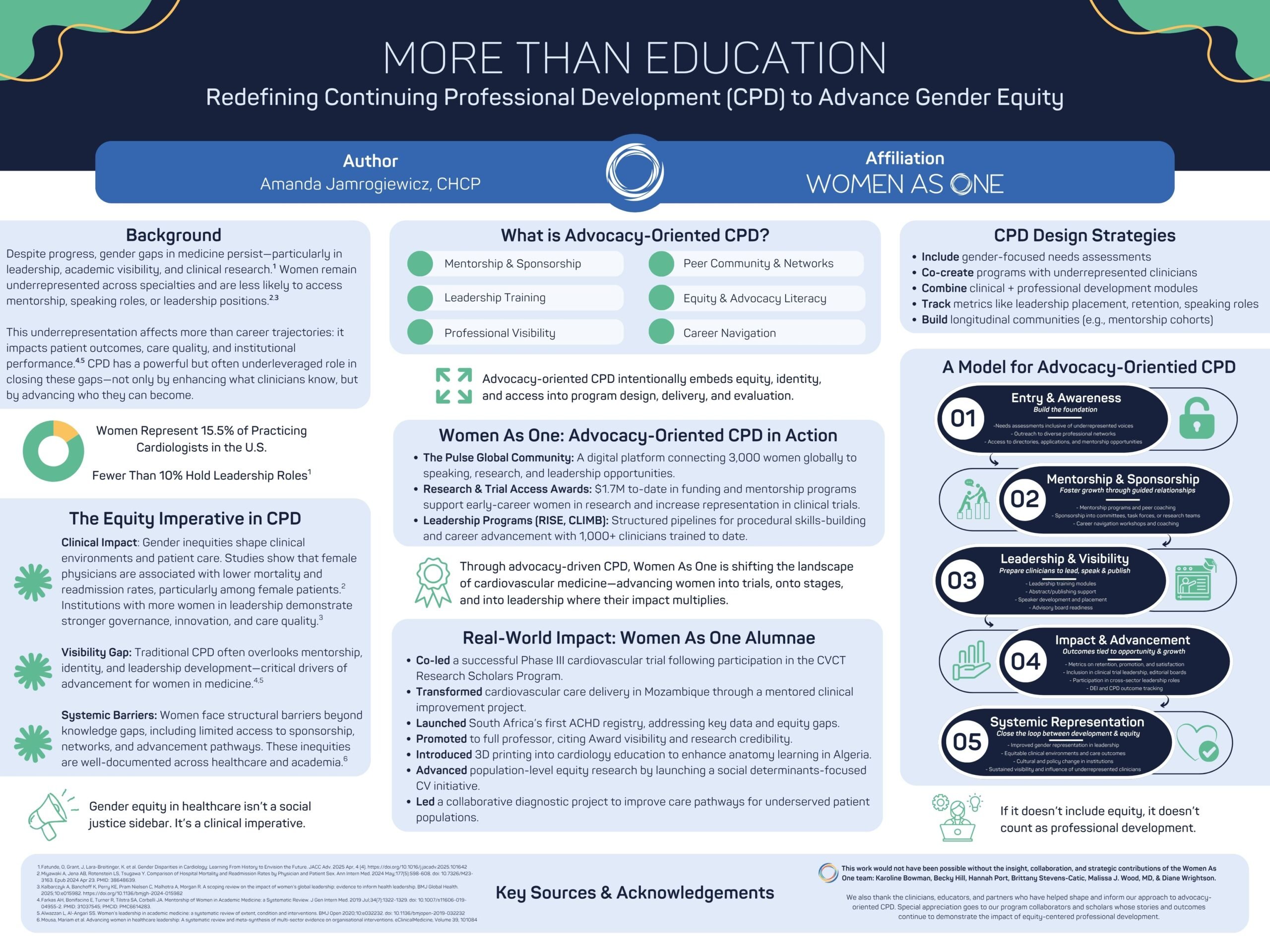
At the 2026 Alliance Annual Conference, Women As One presented a poster that asked a powerful question: What if continuing professional development (CPD) did more than teach clinical knowledge— and instead helped shape the future of the workforce itself?
For decades, professional education in medicine has focused primarily on what clinicians know and how they practice. That work remains essential.
But persistent gender gaps across cardiology—from leadership positions to research participation and speaking opportunities—demonstrate that knowledge alone is not enough to ensure equitable advancement.
To truly strengthen the field of cardiology, professional development must also support who clinicians become, the opportunities they access, and the voices that shape the future of cardiovascular medicine.
Our poster, More Than Education: Elevating Equity and Identity Through CPD, explores how a new model of advocacy-orientated CPD can help close these gaps.
Advocacy-orientated CPD expands the traditional model of professional education. In addition to building clinical expertise, it intentionally supports the structural elements that shape career advancement—mentorship, sponsorship, leadership development, visibility, and professional networks.
By integrating these elements into professional education, CPD can become a powerful engine for advancing equity—and ultimately improving patient care.
Why this matters
Gender inequities in medicine are not simply workforce issues. They influence research priorities, clinical trial representation, leadership decision-making, and ultimately the care patients receive.
When women clinicians have equitable opportunities to lead, research, and shape clinical practice, the entire healthcare system benefits.
Yet structural barriers remain. Women physicians often have less access to mentorship, sponsorship networks, and leadership pathways—factors that are critical for career advancement.
This is where advocacy-orientated CPD comes in.
By intentionally designing programs that foster mentorship, build leadership skills, create visibility, and support long-term professional growth, organizations can help ensure that the next generation of cardiovascular leaders reflects the diversity of the patients they serve.
Turning opportunity into impact
Since its founding, Women As One has supported thousands of women cardiologists across more than 100 countries, expanding access to mentorship, research opportunities, and leadership development.
Through programs like CLIMB, RISE, Mentorship Awards, and our global digital community, The Pulse, thousands of women cardiologists have gained mentorship, leadership training, and opportunities that accelerate their careers and expand their influence.
Today, the outcomes of these programs are shaping the field in tangible ways:
- Women As One alumnae are leading clinical trials and advancing cardiovascular research
- Clinicians supported through our programs are building registries, launching new care models, and expanding access to specialized care
- Women cardiologists are gaining greater representation on speaker panels, advisory boards, and leadership pathways
- A global community of more than 3,000 women cardiologists is strengthening collaboration, mentorship, and visibility across the profession
These outcomes demonstrate what becomes possible when professional development goes beyond traditional education to intentionally support leadership, identity, and community.
A call to the cardiovascular community
Advancing equity in cardiology is not the responsibility of one organization—it requires a collective effort across the entire ecosystem of clinicians, educators, institutions, and industry partners.
For women cardiologists, this means engaging in the programs, mentorship networks, and leadership opportunities that help shape the future of the field. Whether through CLIMB, RISE, research initiatives, or participation in The Pulse community, your involvement strengthens a growing movement dedicated to advancing women in cardiology.
For our partners and supporters, this work demonstrates the powerful impact that strategic investment in equity-focused professional development can have on the workforce and the patients we ultimately serve.
Together, we can redefine what professional development looks like in medicine—not just as a pathway for learning, but as a catalyst for leadership, opportunity, and lasting change.
Explore the poster
We invite you to explore the poster below (click here to download it) to learn more about the evidence, framework, and real-world impact behind this work—and to join us in continuing to expand what professional development can achieve for the future of cardiovascular medicine.
Learn more about Women As One at womenasone.org










{kind=link}

 News2 weeks ago
News2 weeks agoOvum secures US$4m in seed funding

 Entrepreneur2 weeks ago
Entrepreneur2 weeks agoXella launches AI-powered precision health platform

 Insight2 weeks ago
Insight2 weeks agoMost IVF add-ons not backed by reliable evidence, research finds

 Fertility2 weeks ago
Fertility2 weeks agoImmunotherapy may temporarily restore fertility in premature menopause

 News2 weeks ago
News2 weeks agoEU committee warns of women’s health ‘blind spot’

 News2 weeks ago
News2 weeks agoDon’t miss HTW’s upcoming deep dive into health AI
 Insight2 weeks ago
Insight2 weeks agoChanges in AI mammogram risk scores help predict future breast cancer

 AI4 days ago
AI4 days agoBreast cancer biosensor and low-cost ultrasound startups win women’s health AI competition