




News
Ending the guesswork in cancer care: A CEO’s vision for predictive precision oncology

By Wolfgang Hackl M.D., Founder & CEO, OncoGenomX Inc., Switzerland
During my career as an oncologist and cancer drug developer, one question haunted me more than any other: Why do some patients respond to therapy — while others, with the same diagnosis, do not?
We have innovative treatments, biomarkers, advanced lab tests, and guidelines. But far too often, despite all that science, our treatment decisions come down to educated guesswork.
As medicine evolves, so do our data — but not always our ability to act on it with precision.
That enduring gap between what we know and what we can predict inspired me to found OncoGenomX, and to build PredictionStar™, a platform designed to redefine what precision oncology truly means.
From Biomarkers to Behavior: The Missing Link
Today, most molecular cancer tests focus on eligibility: they tell us whether a tumour expresses a particular target or carries a known mutation. This is useful, but it’s only half the story.

Eligibility does not equal efficacy.
Knowing that a patient’s tumour expresses the estrogen receptor (ER), or harbours a PIK3CA mutation, doesn’t mean it will respond to hormone therapy or PI3K inhibition. It simply means those drugs might work. And in oncology, “might” is not enough.
PredictionStar™ was built to close this precision gap — by answering not just which drugs can be used, but which will actually work.
We call this Precision Drug–Tumor Matching: the ability to segregate effective from ineffective treatments by connecting genomic and phenotypic insights into a coherent tumour profile predictive of therapeutic response.
Introducing PredictionStar™: Coherent Biomarker Intelligence
PredictionStar™ is a multidimensional tumour profiling and decision-support system powered by what we term Generative Clinical Intelligence™ — the synthesis of high-quality sequencing data and AI-driven interpretation into clear, actionable clinical guidance.
 Traditional assays analyse biomarkers in isolation, treating each gene mutation or expression pattern as a separate clue.
Traditional assays analyse biomarkers in isolation, treating each gene mutation or expression pattern as a separate clue.
PredictionStar™ instead identifies logically connected biomarker constellations — genomic enablers that reveal which response mechanisms are active, and phenotypic differentiators how likely the tumour will respond.
This networked approach replaces fragmented snapshots with an integrated, functional map of tumour behaviour.
It provides oncologists with something they rarely get from today’s tests: confidence. In clinical modelling, PredictionStar™ has the potential to reduce overtreatment fivefold and lower the cost of achieving one year of tumour growth control by 35 per cent.
But the numbers tell only part of the story. Behind them are patients spared from unnecessary toxicity — and doctors empowered to treat with precision instead of probability.
Built on the Technology of Giants
PredictionStar™ was designed for seamless integration into modern real-world workflows, harmonized and cross-validated to ensure reliability, and reproducibility.

The platform’s pre-sequencing tumor workup is fully standardised, minimizing inter-laboratory variability that can otherwise reach 70 per cent.
From tumour processing to data interpretation, PredictionStar™ enforces the same rigorous quality in every step, producing consistent and concordant results across labs.
As far as cloud architecture optimized for medical data privacy and global scalability we are privileged to work with world class-players of the health IOT industry
(F. Gaede, Oct 2025, Nordcloud).
A Femtech Focus: Personalising Breast Cancer Therapy
While PredictionStar™ has broad oncology applications, our first focus is hormone receptor-positive breast cancer, the most prevalent form among women.
It is here that the limits of current diagnostics are most evident — and the need for predictive and prescriptive clarity is greatest.
 Even within hormone-dependent breast cancer, the most favorable form of the disease, patient outcomes vary widely. Some women respond beautifully to endocrine therapy for years, while others progress rapidly.
Even within hormone-dependent breast cancer, the most favorable form of the disease, patient outcomes vary widely. Some women respond beautifully to endocrine therapy for years, while others progress rapidly.
What makes the difference? The answers are buried in the tumour’s individual response profiles — but until now, we lacked the tools to decode them. PredictionStar™ offers that decoding ability.
Our non-interventional validation study, conducted in collaboration with clinical researchers from the Veterans Affairs Medical Centers in Cincinnati, Los Angeles, and Miami, involves data from over 4,300 patients with hormone receptor-positive disease.
By correlating predicted responses with actual treatment outcomes, we aim to establish a new clinical standard for predictive accuracy.
Our roadmap includes RUO and LDT certification in 2026, FDA-IDE clearance in Q2 2027, first RUO test sales as early as Q1 2027, and clinical study use from Q3 2027 onwards.
Redefining Precision Oncology
To understand why this matters, we need to reframe what “precision” means.
Most tests today are prognostic or eligibility-based. They classify risk or confirm target presence. PredictionStar™ adds a third, transformative dimension: functional prediction. It asks, “Which therapies will this specific tumour respond to — and how strongly?”
This evolution turns diagnostics into a true decision-support tool, enabling oncologists to design treatment compositions optimized for efficacy, rather than constrained by averages.
The distinction may seem subtle, but its impact for individuals living with breast cancer is enormous: Prognostic and eligibility tests describe. PredictionStar™ guides.
Innovation Through Unity
Our strength lies in collaboration.
I’ve often said that OncoGenomX stands “on the technology of giants, powered by the ambition to transform.” That is more than a slogan — it’s our reality. We built PredictionStar™ not as an isolated product, but as a platform for partnership.
Its architecture invites integration — with hospital systems, sequencing providers, AI developers, and pharmaceutical R&D pipelines.
In the coming years, we envision PredictionStar™ evolving into a broader family of tools: PredictionStar DX™ for predictive diagnostics, PredictionStar GCI™ for data integration and generation of actionable clinical intelligence, and PredictionStar IOT™ for real-time connectivity. Each module serves the same purpose: to transform complexity into clarity.
From Data to Decisions: A Personal Reflection
At its heart, PredictionStar™ was born from empathy.
As a clinician, I saw too many patients fall through the cracks — not because we lacked treatments, but because we lacked foresight.
Data without interpretation is noise. Our mission is to turn that noise into understanding.
When I speak with oncologists today, I sense both excitement and relief: “We will no longer be limited to maybes.” “We can begin to quantify response likelihood, combine therapies more rationally, and give patients something we cannot give today: certainty”.
Technology can be transformative, but only when anchored in purpose. For OncoGenomX, that purpose is simple — to give every patient the best possible chance at lasting response.
The Road Ahead
Our journey is just beginning. We are validating, scaling, and expanding across cancer types — from breast to prostate, lung, and beyond.
But our guiding principle remains unchanged: wherever there is cancer, there is a need for precision drug–tumour matching.
The convergence of genomics, phenomics, AI, and clinical data is redefining healthcare.
PredictionStar™ is part of that transformation — proving that predictive precision is not a futuristic concept, but an attainable standard.
We owe it to patients, to clinicians, and to science itself to make that standard universal.
In Closing
When I founded OncoGenomX, I imagined a world where no cancer patient has to live with uncertainty — where treatment is guided by prediction, not probability.
Today, that world feels within reach. PredictionStar™ is more than technology. It’s a promise:
That every patient deserves clarity. That every tumour can be understood.
And that, together, we can end the guesswork in cancer care.
Contact: Dr. Wolfgang Hackl | Founder & CEO, OncoGenomX | E-Mail | LinkedIn WH | Company Webpage | LinkedIn OGX












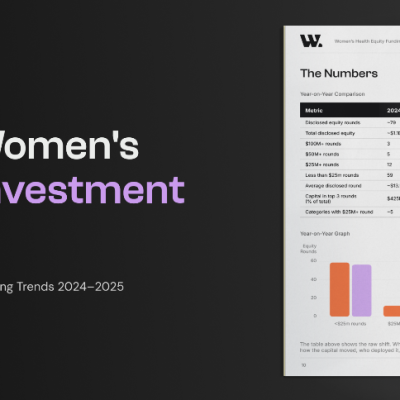
Women’s health has become one of the most searched and shared topics online, from cycle syncing and cortisol management to menopause hacks, supplements, hormone testing and clinician-creator content.
That surge in attention, sometimes dubbed “healthmaxxing,” is changing how women find, evaluate and act on health information, and it is starting to reshape the relationship between patients, clinicians and the companies building products for this market.
For providers, the shift means patients are arriving better informed but also more exposed to unverified claims, putting pressure on clinicians to engage with online narratives rather than dismiss them.
For femtech and pharma companies, it opens a route to reach and educate consumers at scale, but also raises the stakes on credibility: products and messaging that ride the trend without clinical grounding risk eroding the trust the industry has spent years building.
Investors are watching the same dynamic from a different angle.
Attention-driven demand can be a signal of where the next wave of femtech growth will come from, but distinguishing genuine clinical need from viral momentum is increasingly part of due diligence.
The net effect is a widening gap between companies that treat cultural attention as a distribution channel for credible, evidence-based care, and those that risk being swept up in trends with little clinical substance behind them.
How that gap plays out will shape patient trust, clinical relationships and commercial opportunity across the women’s health industry for years to come.
These themes will be explored in more depth in an upcoming webinar, “Women’s Healthmaxxing: The Opportunity & Risks of Cultural Attention for the Women’s Health Industry,” hosted by the Women’s Health Innovation Summit (WHIS), featuring Ellen Wilcox (Listen Ventures), Jessica Bell van der Wal (Frame Fertility), Dr. Tosin Sotubo-Ajayi (NHS, BBC and more) and Nora Lansen (Elektra Health).
Register free for the webinar on 23 July 2026 at https://events.virtualpro.com/womens-health-series-webinar-july-2026/registration

More young midwives are leaving the NHS before 35 as burnout adds pressure to stretched maternity services, new research has revealed.
The trend has raised concerns about the quality and safety of care for mothers and babies in understaffed maternity units.
During 2025-26, 1,669 midwives aged 34 or under left the health service in England, representing 57 per cent of the 2,949 midwives of all ages who resigned.

The pressures of maternity care, including increasingly complex childbirth and the risks involved, are thought to be among the factors behind the trend.
Hannah Leonard, deputy chief midwife at the Royal College of Midwives, said the exodus of midwives under 35 was “deeply worrying” and showed that too many were ending up “burnt-out within a few years of qualifying because every shift means too few colleagues, missed breaks and unpaid hours”.
She added: “Losing these midwives, and students, even before they qualify, is a terrible waste of talent.”
The figures, revealed in parliamentary questions tabled by the Liberal Democrats, show that 205 of last year’s younger leavers were under 25, while 655 were aged 25 to 29 and 809 were aged 30 to 34.
The number of midwives under 35 leaving the NHS has risen sharply in recent years. The 2025-26 figure was 59 per cent higher than the 1,051 who left in 2014-15, according to NHS figures.
Burnout means long-term physical and emotional exhaustion, often linked to sustained pressure at work.
Separate figures obtained by the Liberal Democrats suggest almost one in four midwifery students are leaving before completing their three-year degree.
In 2021, 3,565 students started a midwifery degree, but 2,725 graduated in 2024, meaning 840, or 24 per cent, did not complete the course.
Midwifery students spend much of their second and third years learning on the job in maternity units.
The loss of staff and students underlines what the Royal College of Midwives has described as a “staffing emergency” in maternity care across the UK.
A recent survey by the Royal College of Midwives found that three-quarters of midwives had considered leaving the profession over the last year, mainly because of concerns over staffing levels and patient safety.
Both recent large-scale reviews of maternity care in England, led by Donna Ockenden and Valerie Amos, identified staffing shortages as a key problem affecting patient safety.
Helen Morgan, the Liberal Democrat health spokesperson, said: “These statistics reveal an alarming crisis in maternity, with far too many midwives burning out early in their career and in their training. Patients are paying the price, and mothers are left with no alternative but to give birth on understaffed and unsafe wards.
“Rather than throw money at yet more new recruits who quit under intolerable pressure, the government needs a new approach. Through guaranteeing protected, year-round training and professional development we can help midwives cope with rising complexity and risk.”
About 10 per cent of all midwives leave the NHS each year.
However, the figures show higher leaving rates among younger midwives, with one in seven, or 14.6 per cent, of those aged 25 to 29 and one in six, or 16.6 per cent, of those aged 30 to 34 leaving during 2025-26.
A Department of Health and Social Care spokesperson said: “Under this government we have a record number of midwives in the workforce and we value the vital service they provide in maternity and neonatal units across the country.
“To make the NHS the best employer it can be, we have introduced new NHS staff standards to improve health and wellbeing support, promote flexible working, as well as crucial measures to tackle violence, sexual harassment or abuse and racism.
“Alongside consecutive above-inflation pay rises, we’ve bolstered the midwifery workforce through our graduate guarantee and recently opened up 1,000 more midwifery roles backed by £10m to help prevent student midwives leaving the profession.”
Department of Health and Social Care figures show a record 25,500 full-time-equivalent midwives are working in the NHS, 2,000 more than when the Labour government took office in July 2024.

Nearly six in ten young women get health and wellness advice from influencers, new research shows.
Women aged 18 to 29 were more likely than young men to use online influencers for health information.
The topics included beauty, alternative medicine, mental health, weight loss and fitness.
The Pew Research study found that 57 per cent of women aged 18 to 29 said they get health and wellness information from online influencers, 10 percentage points higher than young men.
While Americans still mostly rely on healthcare providers, the research suggests social media influencers also play a major role in how young people find health advice.
Among women who get health and wellness information from influencers, 51 per cent said they often hear about beauty and appearance, compared with 18 per cent of men.
Young women were also around twice as likely as young men to say they see content about alternative medicine, meaning treatments or health practices used outside mainstream medical care.
A third or more of both young men and young women said they often hear about mental health and weight loss from influencers.
Around half or more of both groups said they often see fitness content.
When asked why they seek health and wellness information from influencers, around half of young women said they wanted to make a change to their health or lifestyle.
That compared with 37 per cent of young men.
The research also found that 23 per cent of young women said hearing from people who share their background or beliefs was one reason they used influencers, compared with 14 per cent of young men.
A further 19 per cent of young women said they learnt about things they did not want to ask their doctor, compared with 10 per cent of young men.








 Diagnosis2 weeks ago
Diagnosis2 weeks agoTwo “gamechanger” tests set to speed up endometriosis diagnosis on the NHS

 Insight2 weeks ago
Insight2 weeks agoWomen with PMOS should have annual NHS checks, new guidance says

 News5 days ago
News5 days agoNew menopause drug approved for use by NHS in Scotland

 Cancer2 weeks ago
Cancer2 weeks agoThousands of women could avoid painful cancer exam with new AI blood test

 Entrepreneur2 weeks ago
Entrepreneur2 weeks agoApplications open for the third W Accelerate with Merck KGaA and M Ventures

 Fertility2 weeks ago
Fertility2 weeks agoOlder women face lower chance of fertility treatment working, even with donor eggs, study finds

 News2 weeks ago
News2 weeks agoWe built Ema like a nurse: Here’s why that matters

 News2 weeks ago
News2 weeks agoExperts call for regulation of toxic period product chemicals
1 Comment