




Insight
Danish startup’s tech-enabled jewellery to tackle sexual harassment

With jewellery that doubles as a discreet safety device, Danish startup All U Me is combining social impact with innovation to address the significant impact of sexual harassment on women’s health and wellbeing.
One in three women has experienced physical or sexual violence, and around half have experienced sexual harassment since the age of 15. The misconception that these incidents always occur late at night and in dark alleyways overlooks the reality of these experiences, which for many women are a part of everyday life.
The Government Equalities Office reports that almost 72 per cent of the UK population has experienced sexual harassment at work in their lifetime. Research shows that 56 per cent of women have experienced harassment in gyms, while 60 per cent of women had been harassed while running, and 11 per cent stopped running altogether as a result.
“It’s the everyday experiences that are the problem,” Dorte Caroline Knudsen (pictured above), founder of Danish startup All U Me tells Femtech World.
“It’s not just walking down a dark street in the middle of the night, it’s the everyday, in the supermarket, on the bus, where you experience feeling unsafe or your boundaries not being respected. It’s the mental load that women are expected to carry, almost without talking about it, to get home safely. I can get home safe; I’m not the problem.”
After 14 years as head of products at a Danish software company, at the age of 47, Knudsen felt called to channel her skills into more purposeful entrepreneurship. Inspired by the UN’s Sustainable Development Goals and anger at the global prevalence of gender-based violence, she began looking into what solutions were currently being developed to address it.
“It was sad to see that none of the solutions said anything about prevention,” she says. “All the focus was on normalising what is going on and putting the responsibility on women.”
In response, Knudsen has created a solution that aims to empower women, while also shifting “safety” from an individual to a collective responsibility.
“The beauty of feeling free”
All U Me has designed a range of jewellery featuring delicate gold and silver chains and ocean-inspired charms, which double up as an alarm system to enable them to call for help when they feel unsafe.
“Tech is wonderful, but it can do more when it’s put into something beautiful, which is very rarely seen in the tech space,” says Knusden.
“Most of the existing solutions were one-size-fits-all, but women don’t work like that. We want to wear something that makes us feel beautiful.”
As well as being beautiful to look at, the jewellery is practical. Fully waterproof and with a battery life lasting up to four years, it is designed to be worn all the time, making it “probably the first real wearable”, according to Knusden.
Each item has a discreet button, linked via Bluetooth and GPS to an app connecting the wearer to nearby bystanders. This may be friends or family who have downloaded the app to their phone specifically for this purpose, or other All U Me users in the local area.
If a woman finds herself in an uncomfortable or unsafe situation, three firm pushes of the button notify up to 20 nearby bystanders or ‘backups’ with her location, alerting them to the incident so that they can intervene.
The app trains all users in the 5D bystander intervention method – distract, delegate, delay, direct, document – in as little as three minutes, so they can choose the approach that feels right at the time.
This is designed to break down some of the barriers that may prevent people from stepping in, such as not noticing, not being sure whether help is wanted, or not knowing what to do, Knudsen explains.
“The feedback we get from the workshops we do is that people like to have a framework. Empowering bystanders, by telling them ‘this is what you need to do’, and ‘this is when you need to do it’, makes people a little bit more inclined to help,” she says.

“It’s no more genius than the technology that already exists, and there are times when it might not work, but that’s why the feeling of security is so important, because that’s the everyday benefit of this.”
According to All.u.me’s focus groups, 98.8 per cent of people being trained in these methods feel there’s at least one thing they can do the next time they witness harassment, while 76 per cent who saw harassment after attending the training reported that they intervened.
“The jewellery is just one element,” Knudsen continues.
“It’s actually much more about the feeling of safety and belonging to a community that I hear our users appreciate every day, and the dialogue around it. Maybe it’s telling your loved ones why you want this jewellery, or maybe it’s somebody on the bus, or the bus driver, the bartender, or the guy at the fitness center who has the app. It’s not a guarantee, but that’s where the social responsibility kicks in, and of course, our most important job is to make sure that people have the app.”
Reframing femtech
Safety and sexual harassment can be overlooked in the femtech sector. Both the World Health Organization and the US Centers for Disease Control classify sexual violence as a major public-health issue, and evidence shows that these experiences can not only have a significant impact on mental health but can also lead to physical symptoms and an increased risk of developing chronic conditions, contributing to long-term health disparities.
One recent study found that women who had experienced being stalked and/or obtained a restraining order had a 41 per cent and 70 per cent higher risk of developing cardiovascular disease, respectively. Other research has shown that women with a history of violence are around twice as likely to develop chronic pain conditons and are over-represented among women with conditions such as chronic pelvic pain, IBS, and migraine.
In many ways, All U Me expands the understanding of femtech, centering safety as a foundation for health and equality. But Knusden is wary of being labelled as a ‘femtech’ company.
“The fact that safety is not seen as femtech is quite weird, actually, when statistically so many of us will experience harassment,” she says.
“But I also want to acknowledge that there are so many people who can benefit from this. It’s not just about gender equality, it’s for anybody who may feel unsafe in society.”
Not a jewellery brand, but a tech enabler
The more people who have the app, the more effective the tool is. While women can create their own networks from anywhere by asking friends and family to download the app, it works most effectively in more populated urban areas where more users are likely to be within a 1 km range.
Since launching in June, All U Me now has 2,000 active subscribers in Copenhagen. There are plans to expand into Sweden, Germany, and the UK, but partnerships with existing jewellery brands – to integrate its safety devices into their existing designs – will be crucial for helping this technology reach more women.
“There are so many jewelry brands in the world, I don’t want to be another one,” says Knusden.
“We want to be a technology enabler. Our vision is to empower and inspire everyone – people, brands, organisations – to stand against harassment, whether they do it by downloading the app, or partnering with us to make the jewellery. This is how we will scale through these partnerships.”
She has big ambitions, believing All U Me could be the “first social impact unicorn”, combining scalable tech, commercial sustainability, and philanthropy.
“I have global ambitions with this, but I also have philanthropical ambitions, in the sense that I believe that every young girl and woman should be able to feel safe and be who they are, Knusden adds.
Sharing her experience of using All U Me, one woman described her sense of safety as going from a “two to a four out of five”.
“Her feeling of safety doubled,” Knusden emphasises. “It’s not a 100 per cent guarantee, but it meant that she stopped carrying her keys between her fingers. If we can make people feel safer, and if we can make it easier for bystanders to act, then we can change the world.”









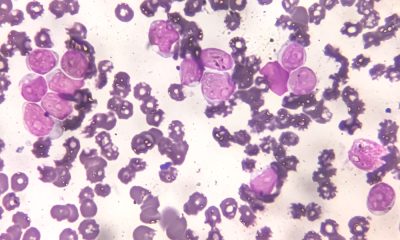

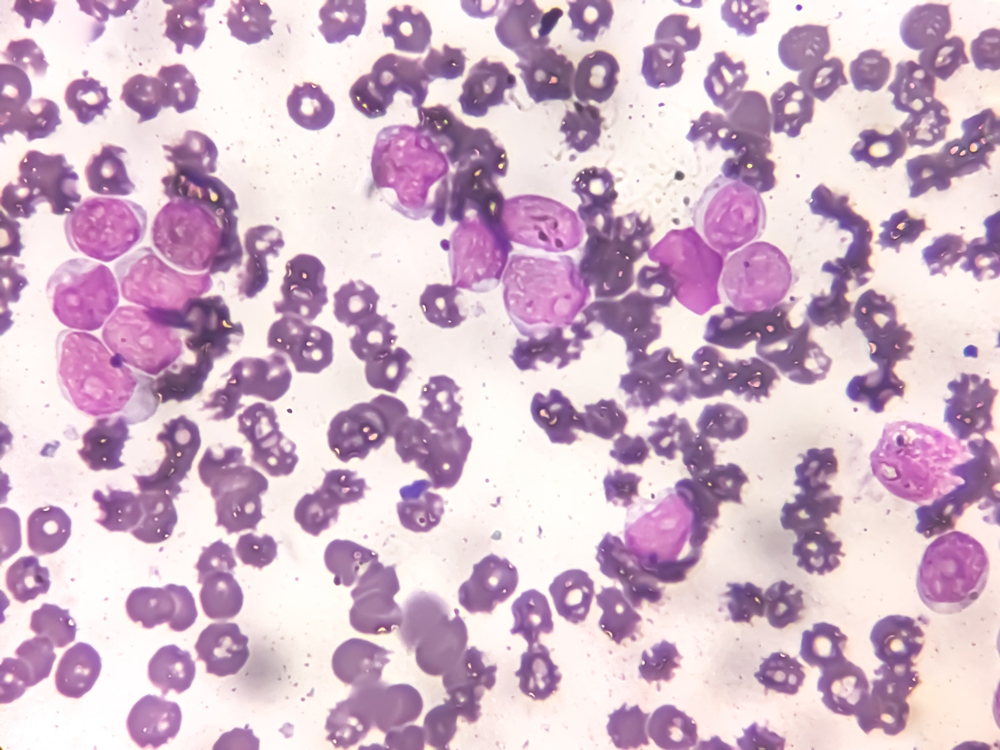
Cancer cells may hijack a fertility protein to repair damaged DNA and survive chemotherapy, research suggests.
The findings could point to a way of making existing cancer treatments more effective.

SYCP1 is a protein normally involved in producing sperm and eggs.
Researchers at the University of Liverpool found that the protein, previously thought to work only in reproduction, can be reactivated in cancer cells, where it helps tumours survive and grow.
SYCP1 usually helps chromosomes pair during meiosis, the form of cell division that produces reproductive cells.
In cancer cells, however, the protein appears to take on another role. It enters the nucleus, the cell’s control centre, binds directly to DNA and regulates genes involved in cell division and DNA repair.
DNA repair is how cells fix damage to their genetic code. In cancer, this process can help tumour cells survive treatment.
The researchers found that removing SYCP1 made cancer cells much more sensitive to chemotherapy drugs that damage DNA.
The findings suggest cancers may use SYCP1 to repair damage caused by treatment and continue growing.
Dr Urszula McClurg, lecturer in biochemistry, cell and systems biology at the University of Liverpool, said: “Our findings show that cancer cells can hijack proteins that normally exist only in reproductive tissues and give them completely new jobs.
“Understanding these unexpected functions opens up exciting opportunities to develop new treatments that make existing cancer therapies more effective.”
The work challenges the long-held belief that proteins active only in fertility have no biological relevance outside the reproductive system.
Researchers say these specialised proteins could provide new treatment targets across many types of cancer.
The study also offers a new view of how cancers evolve by repurposing developmental and reproductive processes.
The findings highlight SYCP1 as a candidate for future precision cancer therapies, which are treatments based on the specific biology of a patient’s cancer.

Women’s health has become one of the most searched and shared topics online, from cycle syncing and cortisol management to menopause hacks, supplements, hormone testing and clinician-creator content.
That surge in attention, sometimes dubbed “healthmaxxing,” is changing how women find, evaluate and act on health information, and it is starting to reshape the relationship between patients, clinicians and the companies building products for this market.
For providers, the shift means patients are arriving better informed but also more exposed to unverified claims, putting pressure on clinicians to engage with online narratives rather than dismiss them.
For femtech and pharma companies, it opens a route to reach and educate consumers at scale, but also raises the stakes on credibility: products and messaging that ride the trend without clinical grounding risk eroding the trust the industry has spent years building.
Investors are watching the same dynamic from a different angle.
Attention-driven demand can be a signal of where the next wave of femtech growth will come from, but distinguishing genuine clinical need from viral momentum is increasingly part of due diligence.
The net effect is a widening gap between companies that treat cultural attention as a distribution channel for credible, evidence-based care, and those that risk being swept up in trends with little clinical substance behind them.
How that gap plays out will shape patient trust, clinical relationships and commercial opportunity across the women’s health industry for years to come.
These themes will be explored in more depth in an upcoming webinar, “Women’s Healthmaxxing: The Opportunity & Risks of Cultural Attention for the Women’s Health Industry,” hosted by the Women’s Health Innovation Summit (WHIS), featuring Ellen Wilcox (Listen Ventures), Jessica Bell van der Wal (Frame Fertility), Dr. Tosin Sotubo-Ajayi (NHS, BBC and more) and Nora Lansen (Elektra Health).
Register free for the webinar on 23 July 2026 at https://events.virtualpro.com/womens-health-series-webinar-july-2026/registration

More young midwives are leaving the NHS before 35 as burnout adds pressure to stretched maternity services, new research has revealed.
The trend has raised concerns about the quality and safety of care for mothers and babies in understaffed maternity units.
During 2025-26, 1,669 midwives aged 34 or under left the health service in England, representing 57 per cent of the 2,949 midwives of all ages who resigned.

The pressures of maternity care, including increasingly complex childbirth and the risks involved, are thought to be among the factors behind the trend.
Hannah Leonard, deputy chief midwife at the Royal College of Midwives, said the exodus of midwives under 35 was “deeply worrying” and showed that too many were ending up “burnt-out within a few years of qualifying because every shift means too few colleagues, missed breaks and unpaid hours”.
She added: “Losing these midwives, and students, even before they qualify, is a terrible waste of talent.”
The figures, revealed in parliamentary questions tabled by the Liberal Democrats, show that 205 of last year’s younger leavers were under 25, while 655 were aged 25 to 29 and 809 were aged 30 to 34.
The number of midwives under 35 leaving the NHS has risen sharply in recent years. The 2025-26 figure was 59 per cent higher than the 1,051 who left in 2014-15, according to NHS figures.
Burnout means long-term physical and emotional exhaustion, often linked to sustained pressure at work.
Separate figures obtained by the Liberal Democrats suggest almost one in four midwifery students are leaving before completing their three-year degree.
In 2021, 3,565 students started a midwifery degree, but 2,725 graduated in 2024, meaning 840, or 24 per cent, did not complete the course.
Midwifery students spend much of their second and third years learning on the job in maternity units.
The loss of staff and students underlines what the Royal College of Midwives has described as a “staffing emergency” in maternity care across the UK.
A recent survey by the Royal College of Midwives found that three-quarters of midwives had considered leaving the profession over the last year, mainly because of concerns over staffing levels and patient safety.
Both recent large-scale reviews of maternity care in England, led by Donna Ockenden and Valerie Amos, identified staffing shortages as a key problem affecting patient safety.
Helen Morgan, the Liberal Democrat health spokesperson, said: “These statistics reveal an alarming crisis in maternity, with far too many midwives burning out early in their career and in their training. Patients are paying the price, and mothers are left with no alternative but to give birth on understaffed and unsafe wards.
“Rather than throw money at yet more new recruits who quit under intolerable pressure, the government needs a new approach. Through guaranteeing protected, year-round training and professional development we can help midwives cope with rising complexity and risk.”
About 10 per cent of all midwives leave the NHS each year.
However, the figures show higher leaving rates among younger midwives, with one in seven, or 14.6 per cent, of those aged 25 to 29 and one in six, or 16.6 per cent, of those aged 30 to 34 leaving during 2025-26.
A Department of Health and Social Care spokesperson said: “Under this government we have a record number of midwives in the workforce and we value the vital service they provide in maternity and neonatal units across the country.
“To make the NHS the best employer it can be, we have introduced new NHS staff standards to improve health and wellbeing support, promote flexible working, as well as crucial measures to tackle violence, sexual harassment or abuse and racism.
“Alongside consecutive above-inflation pay rises, we’ve bolstered the midwifery workforce through our graduate guarantee and recently opened up 1,000 more midwifery roles backed by £10m to help prevent student midwives leaving the profession.”
Department of Health and Social Care figures show a record 25,500 full-time-equivalent midwives are working in the NHS, 2,000 more than when the Labour government took office in July 2024.











 News1 week ago
News1 week agoNew menopause drug approved for use by NHS in Scotland

 Cancer2 weeks ago
Cancer2 weeks agoThousands of women could avoid painful cancer exam with new AI blood test

 Entrepreneur2 weeks ago
Entrepreneur2 weeks agoApplications open for the third W Accelerate with Merck KGaA and M Ventures

 Opinion2 weeks ago
Opinion2 weeks agoWe built Ema like a nurse: Here’s why that matters

 Hormonal health6 days ago
Hormonal health6 days agoStardust period tracker shares health data, study reveals

 News1 week ago
News1 week agoWomen’s health draws record $1.55bn in equity as capital spreads beyond the mega-rounds

 News2 days ago
News2 days agoZero Candida market set to reach over US$2 billion by 2030 – report

 Mental health2 weeks ago
Mental health2 weeks agoSSRIs may lower heat intolerance in women with depression – study
1 Comment