




Opinion
Acceptable data use vs exploitation when women receive ‘free’ digital health tools

By Wolfgang Hackl, CEO, OncoGenomX Inc., Allschwil, Switzerland
In women’s health, “free” digital tools occupy an especially sensitive space. Period trackers, fertility apps, pregnancy platforms, menopause programs, pelvic-floor wearables, contraception reminders, mental-health chatbots and symptom diaries have become essential resources for millions worldwide. For many, these tools fill longstanding gaps in clinical care, offering information, monitoring and community.
Yet women’s health data are uniquely intimate, politically vulnerable and commercially valuable. The same apps that help a woman identify a fertility window or track post-partum mood changes may also collect sexual history, location, device IDs, hormonal patterns, and behavioral clues that can be monetized or repurposed – sometimes without meaningful transparency.
The core ethical question is urgent: When does the data exchange that underpins “free” women’s health tools empower individuals, and when does it exploit them?
Across research and policy commentary, the fault lines remain the same – transparency, proportionality, control, fair value sharing, and protection from harm – but their stakes are heightened in women’s health.
The high-risk profile of women’s health data
The sensitivity of women’s health data is not abstract. It becomes dangerous in real-world contexts:
- Reproductive rights volatility – In jurisdictions with restrictive reproductive laws, menstrual cycle data, geolocation patterns around clinics, search histories and communication logs can be weaponized.
- Stigma and discrimination – Data related to miscarriage, abortion, infertility, menopause symptoms, mental health, sexual function or domestic violence can lead to insurance denial, unfair pricing, employment impacts or social vulnerability.
- Relationship and safety risk – Some apps collect or expose data that partners or third parties could misuse, from mood logs to location traces.
- Commercial targeting – Women are historically targeted with exploitative advertising around fertility supplements, weight loss, anti-aging and alternative therapies, often amplified by intimate behavioral data.
These risks transform the ethics of “free.” When a tool’s business model depends on collecting sensitive reproductive or behavioral attributes at scale, the user is no longer the beneficiary – the user is the product.
What women expect when sharing health data
Studies consistently show broad support among women for sharing data when it drives tangible health benefits—research, better care pathways, early diagnosis, or community insights. Trust collapses when data are:
- shared with advertisers, data brokers or insurers
- used for profiling, risk scoring or targeted pricing
- stored indefinitely or without clarity
- accessible to third parties unknown to the user
Women expect three things above all:
- Radical transparency
Not euphemisms, not hidden trackers, not 30-page terms. Women want to know who sees what, why and how it will be protected.
- Meaningful agency
Granular control – “yes” to sharing anonymized cycle data for research, “no” to targeted ads; “yes” to contributing to public-good datasets, “no” to third-party data inference.
- Safety guarantees
Technical and legal safeguards that explicitly prohibit uses exposing women to legal, financial, physical or psychological risk.
Women’s health is not a sandbox for broad, open-ended data collection. When platforms request permissions unrelated to their core health function – photos, contacts, continuous location, device fingerprinting – alarm bells ring.
Exploitation patterns in “free” women’s health tools
Technical audits of menstrual and fertility apps show that many collect extraordinarily detailed data: cycle length, symptoms, sexual activity, pregnancy intentions, test results, mood logs, sleep, stress, location, device IDs, email metadata, and “other information.” Some share with dozens of third parties.
The exploitation signals are increasingly well understood:
- Opaque data pipelines to marketers, analytics firms and profiling engines
- Unbounded storage of sensitive reproductive histories
- Engagement-driven design that nudges users toward disclosing more
- Commercial re-use of intimate behavioral patterns unrelated to health
- Minimal or performative governance despite high-risk categories
When a woman logs cramps or sexual activity, the ethical baseline is higher than in general wellness apps. The potential harms – legal, social, relational – are uniquely gendered and often irreversible.
Value capture and the “women pay twice” problem
Women’s health technologies have become a multi-billion-dollar market. But the value chain often flows upward, not back to the users:
- Women supply intimate, high-granularity data – Immense value for R&D, precision marketing, and investor storytelling.
- Companies monetize the insights – Through partnerships, advertising, risk scoring or AI model development.
- Women then purchase the resulting products – Including paid upgrades, supplements, or premium diagnostics whose innovation was subsidized by their data.
Without mechanisms that guarantee affordability, open reporting or reinvestment into women’s health services, the model becomes extractive. Women contribute the raw material, then buy back the finished product at retail price.
Pathways to acceptable – and truly empowering – data use
Responsible data practice in women’s health requires stricter standards than generic “digital health ethics.” The following markers – derived from current scholarship—are especially critical in women’s health contexts:
- Purpose-bound data practices
Tools should collect only what is strictly necessary for the health purpose. Fertility predictions do not require contact lists or persistent location tracking.
- Prohibitions on harmful secondary uses
Contracts and code must explicitly block:
- insurance scoring
- law enforcement access without due process
- targeted advertising linked to reproductive data
- cross-platform tracking
- sale to data brokers
- High-security architecture
Women’s health data should be treated like genomic or mental health data:
- encryption at rest and in transit
- zero-trust design
- independent security audits
- strict third-party access regimes
- Governance designed for vulnerable contexts
Oversight bodies should include women’s health experts, legal scholars, and patient advocates, reviewing not just privacy compliance but real-world harm potential.
- Fair value and reciprocity
If population-level reproductive or maternal health data fuel AI models, companies should commit to:
- affordability of products derived from those models
- investment in community health infrastructure
- transparency in data-driven improvements
This is not charity. It is ethical reciprocity.
The way forward: trust as a differentiator
Women’s health is evolving from niche to mainstream. With this visibility comes responsibility. Investors and innovators who treat data stewardship as a strategic asset – not a compliance hurdle—will define the next era of digital women’s health.
The future belongs to tools that:
- put safety ahead of scale
- align business models with women’s interests
- eliminate dark patterns
- prove that “free” does not mean “exploitative”
- create value with, not from, women
Ultimately, the line between acceptable data use and exploitation is shaped by one question:
Does this tool treat women as partners—or as data sources?
The companies that choose the former will earn the trust that defines the next generation of global women’s health innovation.














By Women As One
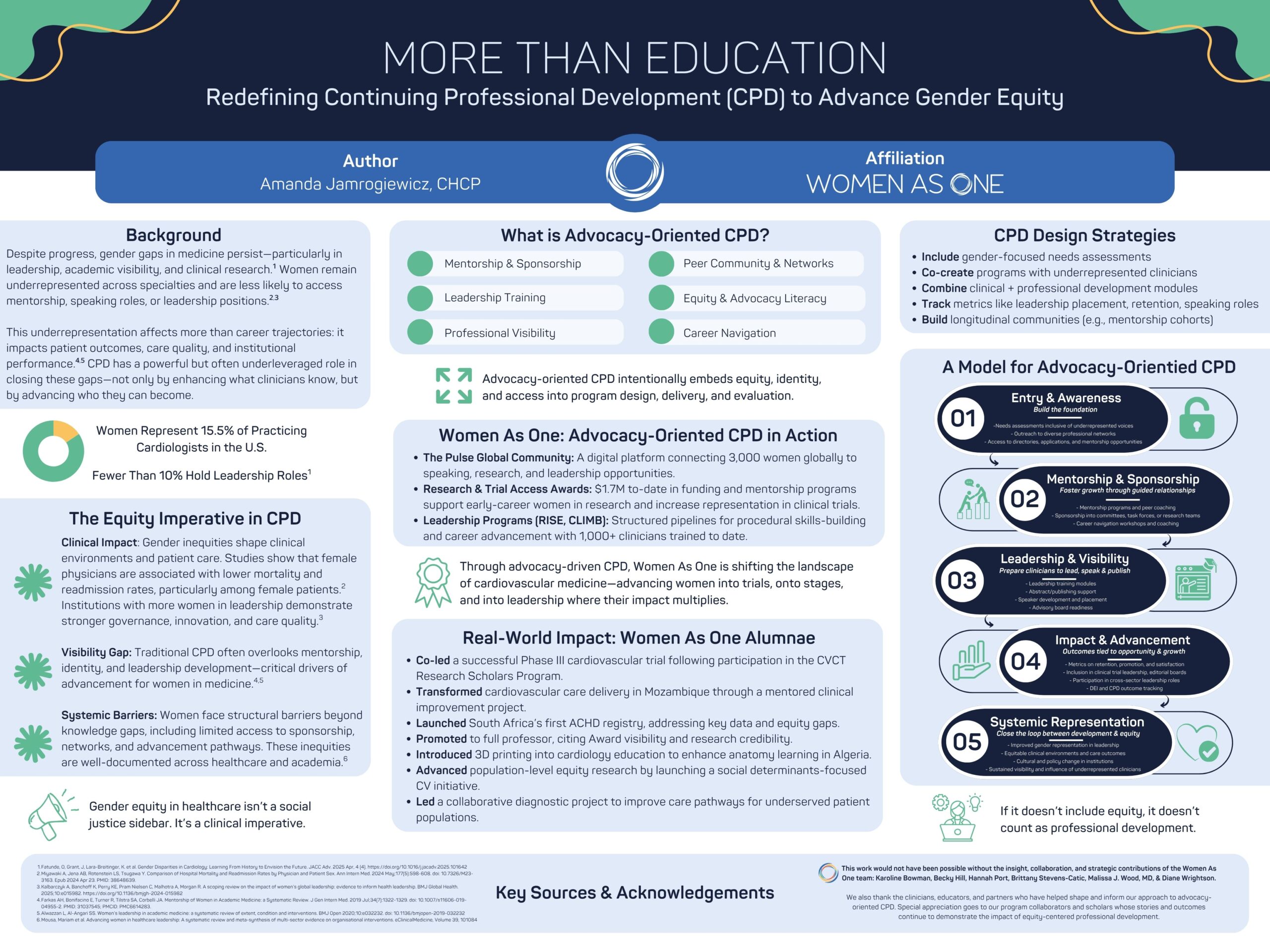
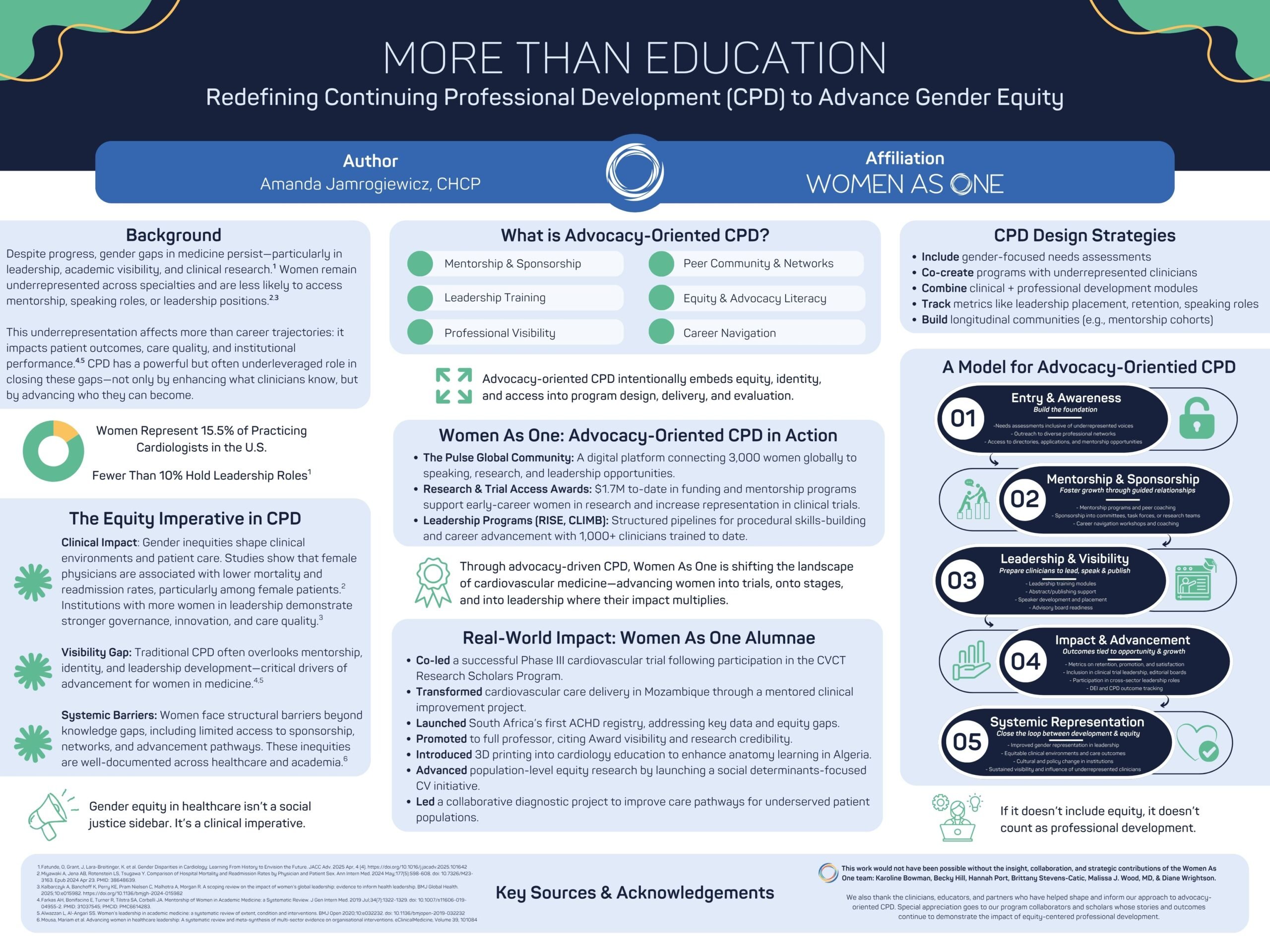
At the 2026 Alliance Annual Conference, Women As One presented a poster that asked a powerful question: What if continuing professional development (CPD) did more than teach clinical knowledge— and instead helped shape the future of the workforce itself?
For decades, professional education in medicine has focused primarily on what clinicians know and how they practice. That work remains essential.
But persistent gender gaps across cardiology—from leadership positions to research participation and speaking opportunities—demonstrate that knowledge alone is not enough to ensure equitable advancement.
To truly strengthen the field of cardiology, professional development must also support who clinicians become, the opportunities they access, and the voices that shape the future of cardiovascular medicine.
Our poster, More Than Education: Elevating Equity and Identity Through CPD, explores how a new model of advocacy-orientated CPD can help close these gaps.
Advocacy-orientated CPD expands the traditional model of professional education. In addition to building clinical expertise, it intentionally supports the structural elements that shape career advancement—mentorship, sponsorship, leadership development, visibility, and professional networks.
By integrating these elements into professional education, CPD can become a powerful engine for advancing equity—and ultimately improving patient care.
Why this matters
Gender inequities in medicine are not simply workforce issues. They influence research priorities, clinical trial representation, leadership decision-making, and ultimately the care patients receive.
When women clinicians have equitable opportunities to lead, research, and shape clinical practice, the entire healthcare system benefits.
Yet structural barriers remain. Women physicians often have less access to mentorship, sponsorship networks, and leadership pathways—factors that are critical for career advancement.
This is where advocacy-orientated CPD comes in.
By intentionally designing programs that foster mentorship, build leadership skills, create visibility, and support long-term professional growth, organizations can help ensure that the next generation of cardiovascular leaders reflects the diversity of the patients they serve.
Turning opportunity into impact
Since its founding, Women As One has supported thousands of women cardiologists across more than 100 countries, expanding access to mentorship, research opportunities, and leadership development.
Through programs like CLIMB, RISE, Mentorship Awards, and our global digital community, The Pulse, thousands of women cardiologists have gained mentorship, leadership training, and opportunities that accelerate their careers and expand their influence.
Today, the outcomes of these programs are shaping the field in tangible ways:
- Women As One alumnae are leading clinical trials and advancing cardiovascular research
- Clinicians supported through our programs are building registries, launching new care models, and expanding access to specialized care
- Women cardiologists are gaining greater representation on speaker panels, advisory boards, and leadership pathways
- A global community of more than 3,000 women cardiologists is strengthening collaboration, mentorship, and visibility across the profession
These outcomes demonstrate what becomes possible when professional development goes beyond traditional education to intentionally support leadership, identity, and community.
A call to the cardiovascular community
Advancing equity in cardiology is not the responsibility of one organization—it requires a collective effort across the entire ecosystem of clinicians, educators, institutions, and industry partners.
For women cardiologists, this means engaging in the programs, mentorship networks, and leadership opportunities that help shape the future of the field. Whether through CLIMB, RISE, research initiatives, or participation in The Pulse community, your involvement strengthens a growing movement dedicated to advancing women in cardiology.
For our partners and supporters, this work demonstrates the powerful impact that strategic investment in equity-focused professional development can have on the workforce and the patients we ultimately serve.
Together, we can redefine what professional development looks like in medicine—not just as a pathway for learning, but as a catalyst for leadership, opportunity, and lasting change.
Explore the poster
We invite you to explore the poster below (click here to download it) to learn more about the evidence, framework, and real-world impact behind this work—and to join us in continuing to expand what professional development can achieve for the future of cardiovascular medicine.
Learn more about Women As One at womenasone.org
Mental health
What Maternal Mental Health Month reveals about where postpartum support actually breaks down

By Morgan Rose, chief science officer at Ema, and Lauren Scocozza, vice president of product at Willow
May is Maternal Mental Health Month, and every year it surfaces a familiar set of statistics: 1 in 5 new mothers experiences postpartum depression or anxiety, most go unscreened, and the majority who are screened don’t receive adequate follow-up care.
The conversation is important. But the numbers obscure something that anyone who has worked in this space knows to be true: postpartum mental health distress rarely arrives with a label.
It arrives as exhaustion. As “I’m not sure I’m doing this right.”
As a question about supply, pumping, whether it’s okay to feel this disconnected from something you were supposed to love immediately.
Willow integrated Ema, AI built for women’s health, with the goal of closing the maternal care and data gap.
The pattern mentioned above appears consistently in Ema’s conversational data through the Willow app.
A mother reports mastitis symptoms.
Ema walks her through the clinical presentation, confirms she should keep pumping, and then she questions if she is using her pump correctly. In the same thread, within a few exchanges, she says she’s “feeling too sad.” Then: “I don’t know. I think I’m depressed. I am not enjoying my postpartum.”
She did not come to the app to talk about her mental health.
She came about a breast infection. The mental health disclosure came through the already-opened door.
The Weight Underneath the Technical Question
New motherhood involves an enormous amount of problem-solving at a time when cognitive and emotional reserves are depleted. The pump has to work. The baby has to eat. The body has to recover.
Work comes back. Sleep doesn’t. Feeding their babies requires skill, and the learning curve sits atop it all.
What Ema’s conversation data shows is that the emotional load of navigating these challenges is not separate from mental health. It is mental health.
When a mother writes, “I’m postpartum and overwhelmed and tired,” and then, in the same breath, asks about flange sizing, she is telling us what the postpartum experience actually feels like from the inside.
The technical question and the emotional state are one and the same.
Breastfeeding carries particular weight here.
The desire to breastfeed, the guilt when it doesn’t go as planned, and the identity questions that come with feeding choices are not peripheral to the postpartum mental health conversation.
In our conversations, women navigating supply concerns often reveal deeper anxieties: about whether they are good mothers, whether their bodies are “working,” and whether the difficulty they are experiencing means something about them.
These are the signals worth asking about.
What Screening Looks Like in Practice
Ema is trained on the Edinburgh Postnatal Depression Scale and is equipped to offer the EPDS when a conversation warrants it.
The value is being present for the moment when a woman is ready to name what she’s feeling.
That moment rarely comes as a direct request for mental health support. It comes when someone is already in a conversation about something else, and something shifts.
A woman dealing with mastitis says she feels sad. A woman worried about supply says she doesn’t feel like herself. A woman managing the logistics of going back to work with a wearable pump says she’s not sure she can keep up with it all — and the “it all” isn’t about the pump.
Ema is designed to hear that. She doesn’t stay on the clinical or technical track when the conversation moves. She follows the person.
And when the moment is right, she offers the screening as a natural next step.
In one exchange, a woman was offered the EPDS after disclosing depressive feelings. She declined.
Ema acknowledged that and asked if she wanted to talk about something else. That’s the right response. The offer was made without pressure. The door stays open.
Sometimes what matters most is that someone asked at all.
The Continuity Problem
One of the most persistent structural failures in maternal mental health care is fragmentation.
A woman sees her OB at six weeks postpartum for a brief screening. She may get a call from a nurse. She may be given a referral she never follows up on because she doesn’t have the capacity to navigate a new care relationship while managing a newborn.
The clinical touchpoints are too few, too far apart, and too often siloed from one another.
The postpartum period lasts far longer than the six-week checkup implies. Mental health symptoms can emerge weeks or months after delivery, shift in character over time, and interact with physical challenges in ways that don’t fit neatly into any single provider’s lane.
A lactation concern becomes an anxiety spiral. A supply drop triggers a grief response. A difficult return to work surfaces a postpartum depression that wasn’t fully recognized at six weeks.
Ema sits inside these moments because she’s embedded in the platform women are already using. She doesn’t require a separate appointment, a referral, or the cognitive bandwidth to seek out a new resource.
She’s in the Willow app that mom is already using multiple times a day to manage her pump.
When Ema identifies a woman who may need more support than she can provide, she routes to the right resource — whether that’s a SimpliFed lactation consultant for feeding-related concerns or a clinical professional for mental health follow-up.
The conversation leads to the handoff with someone who can do more.
What the Month of May Means for the Rest of the Year
Maternal Mental Health Month is a useful moment of attention. The awareness campaigns, the social media posts, and the statistics shared in newsletters matter.
But the gap in postpartum mental health care is not really an awareness problem.
Most people in the perinatal space and beyond know the statistics. The problem is access, timing, and continuity.
AI doesn’t close that gap on its own.
What it can do is be present in the spaces where women already are, at the times when they need something, and attentive enough to recognise that a conversation about a pump, a clogged duct, or a supply concern is also a conversation about how someone is doing.
The question behind the question is often the more important one.
For Willow, the conversation data Ema generates is a map of where mothers are struggling, what they reach for when they need help, and when they are ready to say more than they came to say.
That information, used well, shapes better resources, better onboarding, and a more connected experience across the full arc of the postpartum year and beyond.
Building the infrastructure to support maternal mental health is a year-round project.
Willow is doing one part of that, and the conversations happening on the Willow platform every day are evidence that women want support that meets them where they are… in their app, in their moment, without having to ask for it twice.
About the authors
Morgan Rose is Chief Science Officer at Ema, an AI platform for women’s health. Ema partners with healthcare organisations and femtech companies to deliver clinically grounded AI support across the perinatal journey.
Lauren Scocozza is the Vice President of Product at Willow Innovations, Inc. For women by women, Willow is building a maternal care platform to address the interconnected challenges of postpartum.

By Wolfgang Hackl, MD, CEO OncoGenomX, Allschwil, Switzerland
FemTech is moving from a promising niche to a foundational part of modern healthcare.
Over the next decade and beyond, its real promise will not only be better products, but a more equitable system: one where women’s health is treated as an equal area for innovation, investment, clinical care, and public policy.
That shift matters because women’s health has long been under-researched, underfunded, and too often managed through systems that were not designed with female biology and life stages in mind.
The opportunity now is to change that trajectory.
If stakeholders act deliberately, FemTech can become a category that improves outcomes, expands access, and creates measurable value across the HealthTech ecosystem.
From niche to infrastructure
The most important change ahead is a mindset shift. FemTech should no longer be seen as a narrow consumer segment focused only on logging symptoms.
It should be understood as health infrastructure spanning puberty, fertility, pregnancy, postpartum recovery, menopause, pelvic health, chronic disease, mental health, and long-term preventive care.
This broader framing creates a more durable market and a stronger social case. It also encourages innovation that serves people across the full life course, rather than only at highly visible moments.
In practical terms, this means building tools that are clinically relevant, integrated into care pathways, and designed to work for different populations and health systems.
What needs to change
For FemTech to become a truly equal healthcare category and a genuine societal priority, several layers need to move together.
First, the evidence base must deepen. More sex-disaggregated data, more women-inclusive clinical studies, and more research on conditions that disproportionately affect women are essential.
Without stronger evidence, product development, diagnosis, reimbursement, and clinical adoption all remain constrained.
Second, policy and regulation must mature. Privacy protections need to be strong enough to build trust in highly sensitive health data.
Regulatory pathways should be clear enough to help innovators bring safe, effective products to market without unnecessary delay.
Reimbursement frameworks also need to evolve so that useful digital tools are not limited to those who can pay out of pocket.
Third, healthcare systems must become more open to integration. The best FemTech products should not sit outside the care journey as standalone apps.
They should connect with clinicians, diagnostics, telehealth, and care coordination so that patients experience continuity rather than fragmentation.
Finally, society needs a broader cultural shift. Women’s health should be discussed as a mainstream public health and economic issue, not as a side topic or a private concern.
That means normalizing conversations around menopause, miscarriage, postpartum health, chronic pain, infertility, and long-term preventive care.
The role of each stakeholder
A healthier FemTech future depends on the full value chain.
Founders and product teams need to design for clinical relevance, usability, and trust. The strongest solutions will be those that solve real problems, use data responsibly, and fit into everyday life and care.
Investors can help by backing long-term value creation rather than only consumer growth. FemTech deserves capital that supports rigorous validation, regulatory readiness, and scalable business models.
Healthcare providers and systems play a critical role in adoption. By integrating FemTech into clinical workflows, they can reduce delays in care, improve monitoring, and make support more continuous and personalised.
Payers and insurers can accelerate access by recognising the downstream value of early intervention, prevention, and better self-management. Coverage decisions will strongly shape which innovations become standard practice.
Policymakers and regulators should create environments where safety, innovation, and privacy coexist. Clear standards and supportive reimbursement policy can make the difference between isolated success and category-wide growth.
Employers and public institutions also have a role. Women’s health affects productivity, retention, and long-term wellbeing, which means workplace benefits and public programs can help expand access and reduce inequity.
FemTech is not only “women for women.” It is “everyone to solve a health and social issue that has been ignored for far too long.”
When stakeholders across the value chain recognise women’s health as a shared responsibility, FemTech moves from a segmented category to a mainstream force for better outcomes, fairer access, and stronger social impact.
Why the upside is larger than the market
The benefit of getting this right is not only commercial.
Better women’s health tools can improve early detection, support self-management, reduce avoidable complications, and lower the burden on social and healthcare systems.
They can also help close persistent gaps in access and outcomes that affect families, workplaces, and economies.
For HealthTech innovators, this is an opportunity to build products that are both mission-driven and scalable. For health systems, it is a chance to improve care quality and efficiency. For society, it is a way to move women’s health from an afterthought to an equal priority.
Actions that will move the field forward
The right direction will not happen automatically. It requires deliberate action across the ecosystem.
- Build products around real clinical needs, not only consumer engagement.
- Invest in women-inclusive research and validation from the start.
- Design privacy and governance into the product architecture.
- Create reimbursement models that reward prevention and continuity.
- Integrate FemTech into mainstream care pathways.
- Expand education for clinicians, employers, and the public.
- Expand the category to the invisible concerns to cover the full range of women’s health needs.
When these actions align, FemTech can mature into something larger than a market category. It can become a model for how health innovation should work: evidence-based, inclusive, trusted, and built to improve lives at scale.
A strong FemTech future is not just possible. It is a practical next step if the ecosystem chooses to treat women’s health as what it truly is: a core healthcare priority and a major driver of innovation.
Table: FemTech Focus Areas
| Field | Approximate number of active solutions/companies |
| Reproductive health & fertility | 120+ |
| Pregnancy & maternal care | 80+ |
| Menstrual health | 60+ |
| General women’s health & wellness | 50+ |
| Diagnostics & monitoring | 45+ |
| Menopause & perimenopause | 40+ |
| Pelvic & uterine health | 30+ |
| Chronic women’s health / integrated care | 30+ |
| Sexual health & wellness | 25+ |
Legend: FemTech is becoming a multi-category healthcare layer. Reports also show that software/apps remain the largest product type overall, while reproductive health continues to dominate as an application area. Best-effort estimates based on category listings, company directories, and market reports, not audited totals.










{kind=link}

 Menopause3 weeks ago
Menopause3 weeks agoPerimenopause misinformation ‘putting women at risk’

 Hormonal health4 weeks ago
Hormonal health4 weeks agoNHS urged to update website following renaming of PCOS

 News3 weeks ago
News3 weeks agoWomen still being failed when they reach menopause, experts say

 Entrepreneur3 weeks ago
Entrepreneur3 weeks agoWomen’s Health Innovation Summit opens submissions for 2026 Innovation Showcase

 Insight2 weeks ago
Insight2 weeks agoBritish women among angriest in Europe, health survey reveals

 News3 weeks ago
News3 weeks agoThree menopause innovators shortlisted for Femtech World Award

 Menopause3 weeks ago
Menopause3 weeks agoSweden eyes domestic production of oestrogen patches amid menopause treatment shortage

 Menopause4 weeks ago
Menopause4 weeks agoLow insulin diet and avoiding four food groups may prevent menopause weight gain