




Entrepreneur
Oura launches women’s health AI model

Oura has launched its first proprietary women’s health AI model to provide personalised insights across reproductive health, the wearable ring maker has said.
The model powers the company’s existing AI chatbot, Oura Advisor, and supports questions spanning the reproductive health spectrum, from early menstrual cycles through to menopause.
It is rolling out through Oura Labs, the company’s opt-in experimental feature hub within the Oura app.

Oura says the women’s health AI model draws on established medical standards, research and knowledge sources reviewed by its in-house team of board-certified clinicians and women’s health experts.
It also analyses biometric signals and long-term trends, including sleep, activity, menstrual cycle, pregnancy and stress data, to tailor guidance.
Ricky Bloomfield, chief medical officer at Oura, said: “This custom model is a fundamental shift in how we responsibly deploy AI in health to meet the needs of our members.
“Women’s health is too complex, and too often overlooked, to rely on one-size-fits-all systems.
“By designing a model specifically for women and grounding it in trusted clinical science and real-world biometric data, we’re setting the standard for how responsible intelligence should be built and expanded across more areas of health, pairing rigorous science with the lived, longitudinal data that makes Oura uniquely powerful.”
The company said the model is intentionally designed to be non-dismissive, reassuring and emotionally supportive, but stressed that the chatbot is not intended to replace a doctor or be used for diagnosis or treatment plans.
The launch comes after Oura said its fastest-growing user segment is women in their early twenties, according to chief commercial officer Dorothy Kilroy.
Oura said the model is hosted entirely on company-controlled infrastructure and that conversations are never shared or sold. Users can access it by opting into Oura Labs within the app.











Women’s health has become one of the most searched and shared topics online, from cycle syncing and cortisol management to menopause hacks, supplements, hormone testing and clinician-creator content.
That surge in attention, sometimes dubbed “healthmaxxing,” is changing how women find, evaluate and act on health information, and it is starting to reshape the relationship between patients, clinicians and the companies building products for this market.
For providers, the shift means patients are arriving better informed but also more exposed to unverified claims, putting pressure on clinicians to engage with online narratives rather than dismiss them.
For femtech and pharma companies, it opens a route to reach and educate consumers at scale, but also raises the stakes on credibility: products and messaging that ride the trend without clinical grounding risk eroding the trust the industry has spent years building.
Investors are watching the same dynamic from a different angle.
Attention-driven demand can be a signal of where the next wave of femtech growth will come from, but distinguishing genuine clinical need from viral momentum is increasingly part of due diligence.
The net effect is a widening gap between companies that treat cultural attention as a distribution channel for credible, evidence-based care, and those that risk being swept up in trends with little clinical substance behind them.
How that gap plays out will shape patient trust, clinical relationships and commercial opportunity across the women’s health industry for years to come.
These themes will be explored in more depth in an upcoming webinar, “Women’s Healthmaxxing: The Opportunity & Risks of Cultural Attention for the Women’s Health Industry,” hosted by the Women’s Health Innovation Summit (WHIS), featuring Ellen Wilcox (Listen Ventures), Jessica Bell van der Wal (Frame Fertility), Dr. Tosin Sotubo-Ajayi (NHS, BBC and more) and Nora Lansen (Elektra Health).
Register free for the webinar on 23 July 2026 at https://events.virtualpro.com/womens-health-series-webinar-july-2026/registration


Juno Bio has secured US$3.8m to expand its diagnostics platform for vaginal health and reproductive care.
The funding round was led by Ada Ventures, with participation from Artesian, Entrepreneur First and Illumina Accelerator.
The women’s health startup said the seed funding will support the launch of its first CLIA-certified sequencing laboratory in Oakland, California, and a new clinical vaginal microbiome and STI test for healthcare providers.
CLIA certification refers to US laboratory standards for testing human samples used in diagnosis, prevention or treatment decisions.

Dr Leighton Turner, co-founder and chief scientific officer of Juno Bio, said: “The vaginal microbiome is still one of the least understood systems in the body at a clinical scale.
“With our lab, we’re starting to build a measurement standard that clinicians can actually use.
“We believe the level of detail from this kind of testing can meaningfully improve how vaginal healthcare is provided.”
The company is developing precision diagnostics for vaginal health, where patients can experience recurring symptoms, inconsistent diagnoses and treatments based on trial and error.
Juno Bio said bringing testing in-house gives it greater control over the process, from sample handling to results, while allowing it to refine its technology and build what it says is one of the largest datasets focused on the vaginal microbiome.
The vaginal microbiome is the community of bacteria and fungi that naturally live in the vagina. Changes in this balance can be linked to infections, symptoms and wider reproductive health issues.
Juno Bio’s newly launched clinical test examines the wider vaginal microbiome and screens for four common sexually transmitted infections, or STIs.
Rather than looking for a single cause, the test is intended to give clinicians a broader picture of what may be contributing to symptoms.
Juno Bio says this matters because multiple infections can occur at the same time and microbiome changes may be linked to fertility, menopause or recurrent infections.
Dr Anna Powell of Johns Hopkins said: “Vaginal microbiome testing has the potential to significantly reshape how we understand and manage vaginal health, particularly for patients with recurrent or unexplained symptoms.
“While the field is still evolving, advances in sequencing and data interpretation are moving us closer to a future where more personalised, microbiome-informed care can complement existing diagnostic approaches.”
Check Warner, co-founding partner at Ada Ventures, added: “Juno Bio is setting a new standard for how vaginal health is understood and managed.
“What they’ve built at this stage, with this level of capital efficiency, is exceptional.
“We’re proud to support the team as they scale their clinical infrastructure and continue leading innovation in this critically underserved category.”

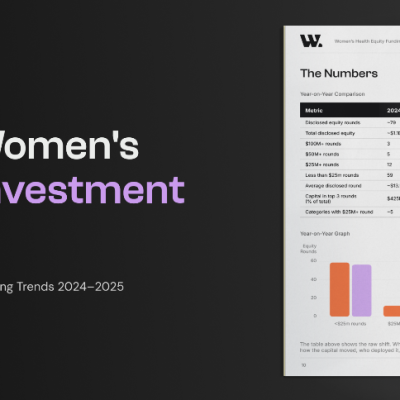
Women’s health companies raised a record $1.55 billion in disclosed equity in 2025, up 41 per cent year on year, according to W Group’s first Global Women’s Health Investment Report, The Road to the Era of Scale.
The report tracks over 500 funding stories and 164 equity rounds across 15 categories and 30+ countries.
Eighty-five companies raised equity in 2025, the highest single-year count on record. But according to the report, the headline figure isn’t the most significant one.
The bigger shift is in where that capital went and how concentrated it was at the top compared to the year before.
The report also points to a brand new investment category that didn’t exist twelve months ago.
SheMed closed a $50 million Series A this year to build a women-specific GLP-1 and metabolic health platform, the first dedicated raise of its kind.
Alongside the momentum, the report identifies one structural risk that could determine whether 2025’s growth holds: a bottleneck at Series A that’s leaving a number of promising seed-stage companies stuck.
Molly Taylor, head of content at W Group, said: “2025 was the biggest year women’s health has ever had, and the most important finding isn’t the headline number.
“It’s that the money has stopped pooling at the top.
“Capital is reaching more companies, more categories and more countries than ever before. The Era of Scale is real. It’s just not finished, and the Series A gap is where it could stall.
“Closing that gap is the highest-leverage move this ecosystem can make in 2026.”
Read the full report: https://wplatform.co/forms/womens-health-equity-funding-trends-report-2026?utm_source=advocacy&utm_medium=ext_email&utm_campaign=2026-q3-health-report-femtech-world








 Diagnosis2 weeks ago
Diagnosis2 weeks agoTwo “gamechanger” tests set to speed up endometriosis diagnosis on the NHS

 Insight2 weeks ago
Insight2 weeks agoWomen with PMOS should have annual NHS checks, new guidance says

 News5 days ago
News5 days agoNew menopause drug approved for use by NHS in Scotland

 Cancer2 weeks ago
Cancer2 weeks agoThousands of women could avoid painful cancer exam with new AI blood test

 Entrepreneur2 weeks ago
Entrepreneur2 weeks agoApplications open for the third W Accelerate with Merck KGaA and M Ventures

 Fertility2 weeks ago
Fertility2 weeks agoOlder women face lower chance of fertility treatment working, even with donor eggs, study finds

 News2 weeks ago
News2 weeks agoWe built Ema like a nurse: Here’s why that matters

 News2 weeks ago
News2 weeks agoExperts call for regulation of toxic period product chemicals
1 Comment