




Events
Cutting through the noise in femtech – key takeaways from Women’s Health Week 2025

The flagship women’s health summit brought together over 400 visionary founders, funders and innovators, with a shared mission of transforming women’s health worldwide.
This year’s Women’s Health Week, which took place at the Barbican, London from 14-17 October, showcased a sector once considered by funders to be too much of a ‘niche’, meeting a crucial unmet need with huge market demand.
Investments are outperforming their value, regulators want to speed up the route to market, and clinical validation is cutting through the noise and demonstrating real results.

There is a buzz about the femtech sector – or at least there was in the Barbican last week – but experts have urged founders should move forward responsibility, building ethics and equity into their innovations.
Here’s our takeaways from the key conversations at Women’s Health Week.
1. Women’s health is outperforming – but angels and influencers are crucial for raising capital
Investment in women’s health is outperforming, and this trend is expected to continue, according to the panel at Women’s Health Week on Thursday 16th, where fund managers and founders highlighted significant returns, growing institutional interest, and the critical role of early-stage backers.
Sanji Chotai, a senior investment manager at British Business Bank, says she is seeing “really encouraging data” and anticipates more “outperformance”, particularly in medtech, which is drawing interest thanks to “shorter timelines to regulatory approval” and rapid commercialisation.
Series A and B activity is also picking up, but the panel agreed that early-stage capital and angel investors remain essential.
“My first angel investment in a women’s health company, I think on Series A, is going to be 20x on multiple and for our fund, it’s going to be around 9x,” said Trin Linamagi, founding partner at Sie Ventures.
“We need to take bigger bets and double down – and actually put the capital behind these businesses early on.”
Having driven successful campaigns for Soulcycle and Barry’s Bootcamp, Tatum Getty, now a founding general partner at THENA, also highlighted the importance of influencers – and not just on Instagram.
“Who is that person who believes in what we’re building and will tell their friends,” she said.
“Women have not been traditional investors they are more risk averse, smaller investment but bigger impact. They add so much more value than the amount of capital that they contribute.”
2. NICE and new pathways for health technologies
During a discussion on mastering Europe’s regulatory process, a representative from the National Institute for Health and Care Excellence (NICE) outlined how new rules-based approval routes, now being introduced for health technologies, are designed to speed access to innovation.
The body is also better aligning processes with the Medicines and Healthcare products Regulatory Agency (MHRA) to reduce the time it takes to regulatory approval.
“We’re taking forward the rules-based pathway for health tech,” said Kendall Gilmore, a senior advisor at NICE.
“Developing a model more similar to the medicines pathway, where, for some products, it goes through the MHRA, through NICE and then comes with a recommendation that has a funding mandate attached.”
The pathway, currently being developed will see health technologies assessed in a similar way to medicines with the first products approved from April next year.
NICE currently evaluates only a fraction of the 500,000 technologies used daily in the NHS. While a NICE recommendation is “not mandatory”, it can be a “powerful signal” to the NHS.
NICE is constantly “horizon scanning” for “disruptive products” further down the pipeline and is engaging more directly with innovators, industry associations and international partners to identify promising technologies earlier, and a new early value assessment route is giving promising products a faster track.
“If it meets an unmet need, it should be used with further evidence generation,” Gilmore explained.
“This is particularly relevant for digital health and diagnostics.”
3. Scientific validation is the most effective way to ‘cut through the noise’
In a panel exploring how to “cut through the noise” in femtech, founders were urged to bake credibility into product design from day one, with scientific proof and clinical validation the sharpest differentiator, according to Soun Rakshit, of MV Health.
“You have to spend probably two years going through the R&D process,” said Rakshit.
“That is the best and probably the only way to do it, so that by the time you get regulatory approval, you have already had significant patient feedback and iteration.”
Earning trust also means collaborating with experts who understand the problem, as Helen O’Neil, founder of Hertility, explained.
When in the development stage, O’Neil reached out to professionals, including obstetricians and gynaecologists to understand the right questions to ask based on their “clinical intuition and personal experience”.
Rakshit added: “If we can show true clinical evidence, and it does take time, it is the best way to cut through the noise.”

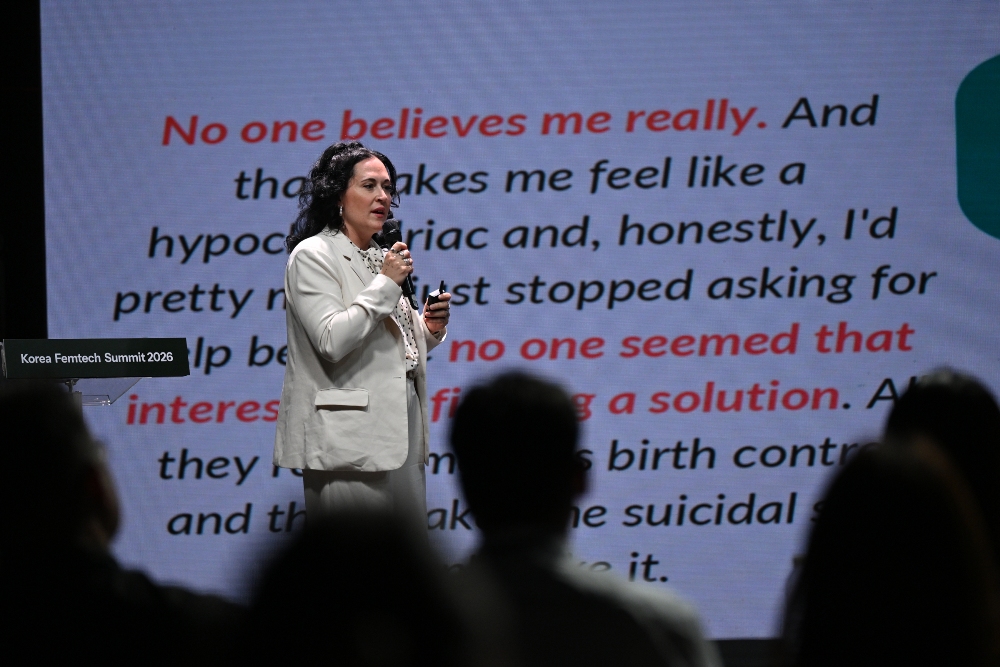
4. Bias in AI is ‘real and harmful’ – and founders need to know how to address it
Experts discussed the role of AI and its potential to both help and harm women’s health, urging proactive testing and human oversight to avoid the risk of decades of a “male default model” being implemented into new solutions.
“AI that’s trained on that skewed data can really fail women,” said Sarah Montgomery Taylor, clinical lead of GenAI evaluation and scaled services at Google, highlighting familiar examples such as heart-attack presentation.
“Biases are real, and they are really harmful, and so being aware of them is so crucial.”
Panellists also flagged “measurement bias” and the “historical dismissal of women’s pain,” where systems trained on those records “can learn to deprioritise” certain signals.
Beyond bias in diagnostics, Marinos Ionnides, head of software and AI medical devices regulation at the MHRA, highlighted the risks of implementing AI in areas where there may be hidden bias.
“I’m quite worried about the deployment of software AI in places where we aren’t we didn’t know we would be finding bias [such as] appointment booking,” he said, adding that in these “unknown unknowns,” “the regulator has their greatest role”.
Founders were urged to be responsible when scaling AI, introducing guardrails such as building in equity and collecting data from the very beginning for “rigorous real-world validation”.
Clinicians need to be able to test the product and understand it to build trust, while regulatory processes should be “adaptive”, offering “clarity on what the path is to market”.
Chen Davies, founder at Anya, shared a real-world example of how products and content tailored for underserved groups drove measurable change, including a “10% population-wise” rise in breastfeeding rates in a deprived area of Blackpool after six months.
“AI should gradually complement human support without replacing it,” said Davies.
5. Consumer data can play a critical role in building the clinical evidence-base
During the final panel, participants argued that continuous real-world data, paired with clinical benchmarks, is the fastest way to fix women’s health’s “male baseline” problem and turn lived experience into evidence.
Dr Chris Curry, clinical director for women’s health at Oura, argued that wearables are “one of the big unlocks” by collecting data that gives the “whole picture of the human”.
But tracking can – should – meet clinical standards, with the panel pushing for globally representative consumer datasets.
“I see consumer data if it’s truly representative, if it’s truly globally representative, being critical,” said Micah Gellman, a senior strategist for women’s health innovation at the Gates Foundation.
“It helps us calibrate and link consumer insights and lived experience to clinical anchors and value outcomes… this kind of consumer data is one avenue that we have to really change investor appetite.”
Rhiannon White, CEO of Clue, which has a long-running research collaboration with Oura, including collecting symptom tracking data on perimenopause and pain, added that women’s spending power can actually steer where future R&D should be focused.
“We are able to shape and direct where people will put their research and put their development with our spending power,” she said.
6. The crisis in government support can be an opportunity for more innovative funding pathways
With the Gates Foundation recently committing an additional US$2.5bn for research in women’s health, Gellman also reframed the reduction in government funding for women’s health – such as that seen under the Trump administration in the US – as an opportunity for more innovate financing.
“There is a real opportunity for European and Asian government funding to step up and fill some of those gaps,” said Gellman.
“An opportunity for government funding and philanthropic funding to take new forms and to be partnering in new ways to catalyse innovation and to work with academics and industry players.”
Rather than a binary between grants and VC, the panel highlighted “blended financing mechanisms, venture philanthropy… different kinds of outcome-based financing” with public and philanthropic dollars used “to de risk, early-stage investment”.
Gellman added: “This crisis that we’re in, in terms of government funding is also an opportunity for innovative financing.”
The comments brought the conference full circle, reminiscent of those made earlier in the day, by Tatum Getty, who highlighted: “Women and small amounts of capital, can make a big difference.”













Hosted by Amanda Ducach, CEO, and Morgan Rose, chief science officer, EmaEQ
Healthcare companies have spent the last two years hearing the same advice: get AI into your product. Few have been told what that actually takes.
Most default to the fastest option. Plug in a general-purpose model, wrap it in a chat window, and call the box checked. It looks like progress on a roadmap slide. It rarely holds up once a real patient is on the other end of it.
We’ve spent years building AI specifically for healthcare, and the lesson that keeps repeating itself is simple: accuracy is not the same thing as trust, and trust isn’t something you bolt on after launch. It has to be part of how the system is built from the first line of code, not a feature added once regulators or users start asking questions.
That distinction is the whole reason clinical accuracy gets treated as a checkbox instead of a discipline. A model can sound confident and still be wrong in ways that matter enormously in a health context.
Knowing the difference, and building for it deliberately, is what separates AI that’s genuinely safe for care from AI that’s simply fast to ship.
On July 20th, we’re hosting a live conversation about exactly this: what companies should be paying attention to before they choose an AI to build with, what clinical accuracy really requires, and the pillars we hold every AI system to before it gets anywhere near a patient’s care.
The Healthcare AI Playbook Webinar: July 20th, 1:30-2pm EST, live on LinkedIn.
Register here: https://www.linkedin.com/events/7482643171823509504?viewAsMember=true
If your team is building anywhere near healthcare, or evaluating what’s already in your product, this is the conversation we think the industry needs right now.

From AI embryo analysis in India to couples fertility care launching in the US, Korea’s women’s health startups are going global, and US investors are taking notice.
Vespexx, the femtech company behind couples preconception health platform Soonr, hosted Korea Femtech Summit 2026 on June 30 in Seoul, convening founders, clinicians, and investors from Korea, Singapore, Canada, and Japan to map the global expansion of women’s health technology.
A panel moderated by Kakao Ventures’ Jade Chung, an OB/GYN-turned-investor, captured the summit’s central theme: Korean startups taking on the world. On stage were three companies already building well beyond Korea. Vespexx, led by Co-CEO Scarlett Joowon Jung, is entering the US with Soonr; Kai Health, founded by CEO Hyejun Lee, has deployed its AI embryo-analysis software across more than 120 fertility clinics in India; and Endo Health, represented by the Head of Design Karlie Hyeonjeong Koo, has built Glow, an AI coaching app whose user base is 98% women and which is backed by US investors including a16z. Together they discussed what it takes for Korean startups to compete globally, where AI creates a real edge, and whether “K-femtech” can follow the path of K-beauty onto the world stage.
The program spanned the full arc of women’s health technology. Lindsay Davis, founder of FemTech Association Asia, opened with a look at where Asia’s femtech stands today. Dr. Juhye Lee of Ewha Womans University Mokdong Hospital offered a clinician’s view of how patient needs are shifting, arguing that women’s health is expanding beyond pregnancy and treatment toward care across the entire life course. Boram Bae, Head of Digital Health PM Part at Samsung Electronics spoke to how a consumer platform at global scale can connect women’s everyday health data with life-stage care. And Rimi Lee, head of the Femtech Center at KOSDAQ-listed diagnostics company Sugentech, traced the evolution of hormone testing from results read by eye to AI-assisted analysis, and pointed toward wearable continuous hormone monitoring as the next frontier.
Vespexx Co-CEO Scarlett Joowon Jung presented the company’s “dyadic health” approach on their ‘Soonr’ app, which brings both partners into fertility and preconception care rather than tracking a woman’s data alone, an approach validated by their legacy product, Signaling’s 800,000 users across Asia, as the company prepares for US launch.
The summit also featured Rachel Bartholomew, the Canadian founder of Hyivy Health and Femtech Across Borders, who built her pelvic-health company, and Megumi Kimura of the Japan Women’s Health Innovation Association, who outlined the investment and business models driving Japan’s fast-growing femtech market.

At the summit, Vespexx also announced the launch of Femtech Korea, an industry network intended to connect Korean femtech companies with global markets and partners, and to serve as a bridge for cross-border collaboration.
“Korea has world-class healthcare technology, but femtech has been one of its best-kept secrets,” said Scarlett Joowon Jung, Co-CEO of Vespexx. “The companies on this stage are proof that’s changing. We’re not just building for Korea anymore, we’re building for the world, and we want US partners and investors to be part of that.”
Korea Femtech Summit 2026 was hosted by Vespexx and co-hosted by FemTech Association Asia. The summit was sponsored by Sugentech, with additional support from Innerness and Octolabs.
About Vespexx
Vespexx is a Korean femtech startup and subsidiary of KOSDAQ-listed biotech Sugentech. The company operates Soonr Health, a couples-focused preconception health platform, and its earlier product Signaling has accumulated over 800,000 users. Vespexx is currently expanding into the North American market.
About Femtech Association Asia
FemTech Association Asia is the region’s first and largest specialist advisory and industry network for founders, investors, corporate partners, and ecosystem contributors, with a core focus on improving women’s health through technology solutions.

Women’s Health Week Europe 2026 has released its full programme ahead of the October event at The Emirates Stadium in London on 7–8 October, with 700+ senior decision-makers and 80+ speakers confirmed across what will be the organisation’s most ambitious edition to date.
For the first time, the event will run across two dedicated stages, each built around a distinct set of questions facing the women’s health industry.
The Global Stage takes on the macro forces shaping the sector: where capital is flowing, how AI is transforming diagnosis and treatment, the gender data gap, wearable technology, stigmatised markets, and the policy landscape across Europe.
Confirmed speakers include Merete Clausen (EIF), Frida Polli (MIT), Nichole Young-Lin (Google), Alison Cave (MHRA), Emily Darlington MP, Kerry Buckley (Boots), Tim Davis (LSEG), Henriette Hessen (Verdane), Hillary Ball (Atomico), and Christine Hockley (British Business Bank).
The Scale Stage runs in parallel, focused on execution: how to navigate regulatory approval pathways, survive the valley of death, build the evidence stack that wins payers and partners, implement AI into a women’s health business, and position for acquisition. Sessions include a reverse pitch format, in which corporates and investors pitch to founders, and a founder’s guide to getting acquired.
The programme also includes two Pitch competitions, one per day, across the Consumer & Tech and Medical Devices & Therapeutics categories, with 16 finalists competing on the mainstage in front of the full delegate audience.
Every session is case study-driven, with speakers selected on the basis of having lived the problem they are on stage to solve.
Women’s Health Week Europe 2026 takes place 7–8 October at The Emirates Stadium, London. The full programme is available now.
View the 2026 programme here
Pre-agenda pricing ends 26 June
Tickets are currently available at pre-agenda pricing, with savings of up to £600 off standard pricing. The deadline is midnight on Friday 26 June. After that, prices go up.
Secure your place: https://wplatform.co/summits/womens-health-week-europe-2026?utm_source=advocacy&utm_medium=ext_email&utm_campaign=whw-europe-26-femtech-world#tickets
Also at The Emirates: Women’s Sport Summit 2026
The day before WHW Europe, on 6 October, The Emirates Stadium will also host the inaugural Women’s Sport Summit, a dedicated one-day event bringing together 400+ attendees from across sport, business, and investment. Focused on the commercial side of women’s sport, the Summit covers the full sports cycle: money, product, and market. Where women’s sport means business.








 Diagnosis2 weeks ago
Diagnosis2 weeks agoTwo “gamechanger” tests set to speed up endometriosis diagnosis on the NHS

 Insight2 weeks ago
Insight2 weeks agoWomen with PMOS should have annual NHS checks, new guidance says

 News5 days ago
News5 days agoNew menopause drug approved for use by NHS in Scotland

 Cancer2 weeks ago
Cancer2 weeks agoThousands of women could avoid painful cancer exam with new AI blood test

 Entrepreneur2 weeks ago
Entrepreneur2 weeks agoApplications open for the third W Accelerate with Merck KGaA and M Ventures

 Fertility2 weeks ago
Fertility2 weeks agoOlder women face lower chance of fertility treatment working, even with donor eggs, study finds

 News2 weeks ago
News2 weeks agoWe built Ema like a nurse: Here’s why that matters

 News2 weeks ago
News2 weeks agoExperts call for regulation of toxic period product chemicals
3 Comments