




Opinion
Femtech in 2025: A year of acceleration, and what data signals for 2026

By Celine Vignal, co-founder of Seesaw Health
The past year marked a turning point in femtech.
After a decade of steady progress, 2025 delivered a wave of innovations that pushed women’s health technology into a more mature, data-driven, and clinically integrated era.
From AI-enhanced hormone analytics to nervous-system biofeedback, companies shifted away from generic wellness and moved toward precision, personalisation, and validated outcomes.

With women now representing more than 80 per cent of household healthcare decisions and nearly 50 per cent of the global workforce, the demand for tools that reflect biological realities and not just generalised averages, has never been stronger.
Major Developments in 2025: From Hormone Intelligence to Pelvic Care
One of the most notable advancements in 2025 was the rapid evolution of AI-powered fertility and hormone-tracking technologies.
Fertility platforms expanded beyond ovulation prediction to offer multi-hormone modeling, giving users clearer insights into perimenopause, thyroid interplay, and metabolic patterns.
The industry also saw a surge in devices capable of real-time hormone detection, supporting more personalised care for women across all life stages.
Menopause tech continued its expansion.
What began five years ago as symptom-logging apps has now grown into integrated care platforms offering telehealth, digital coaching, non-hormonal treatment plans, and AI-based flare-up predictions.
Companies are increasingly leveraging longitudinal data to help identify early markers for sleep disruptions, cardiovascular risk, and mood instability, issues that disproportionately affect midlife women yet have historically lacked attention.
Meanwhile, menstrual and pelvic-health technology advanced significantly.
In 2025, startups brought to market more precise ways to monitor menstrual patterns, pelvic floor function, and chronic conditions like endometriosis.
We saw a rise in devices that combine sensor technology with therapeutic guidance. This reflects a deeper shift: women’s health problems long dismissed as “normal” are now being re-examined through a scientific lens, supported by better data and better tools.
Maternal health also benefited from this momentum.
Remote monitoring platforms now help track blood pressure, glucose variability, and stress biomarkers throughout pregnancy and postpartum, improving early detection for conditions like preeclampsia and gestational diabetes.
Importantly, many of these solutions are being built with inclusivity in mind, aiming to reduce disparities that have persisted for decades.
The Role of Nervous-System Data in Personal Health
Throughout 2025, the value of autonomic data—the signals that reflect how the body responds to stress—gained recognition as a critical element of women’s health.
New biosensors and software have made it possible to measure parasympathetic activity in real time, offering a window into how the nervous system modulates inflammation, pain, hormonal stability, and emotional regulation.
This represents a major shift: instead of using stress-reduction apps that rely solely on self-report or generic protocols, people can now see how their body responds physiologically in the moment.
Beyond wellness applications, this kind of data has important potential for chronic conditions that affect women disproportionately.
Autonomic dysregulation plays a role in migraines, IBS, endometriosis, PCOS, anxiety disorders, and perimenopause symptoms.
Tools that help women understand and regulate their stress response could become a critical layer of preventive care.
Predictions for 2026: Relying on Body Data
1. Nervous-system biomarkers will become as common as heart-rate data
In 2026, real-time stress measures, such as vagal tone, respiratory patterns, and autonomic balance, will increasingly appear in wearables and therapeutic devices.
Seesaw Health is one example of this trend, offering sensor-driven insights into parasympathetic activity to personalise breathwork and recovery.
We’re also seeing early signals from devices integrating sensors directly into earbuds and ambient sensors that adapt lighting and sound based on autonomic patterns.
2. Pelvic and menstrual health will enter a precision-care era
Expect more clinical validation and early-detection tools.
Startups are already piloting AI-powered ultrasound analysis for early endometriosis suspicion and pelvic-floor trainers like Perifit that adjust programmes based on muscle response rather than user guesswork.
High-resolution menstrual-mapping platforms will expand beyond risk scoring to offer cycle-specific care recommendations.
3. AI-driven coaching will personalise daily health decisions
Virtual health assistants will combine biological data with contextual signals to offer just-in-time guidance like Maven Clinic.
Some tools are already experimenting with flare-up prediction for PMDD or endometriosis, and with workout-modification engines that adapt intensity based on inflammation, sleep debt, and stress load.
As these models mature, daily self-care routines could become far more adaptive.
4. Menopause platforms will formalise into mainstream care
With over one billion women projected to be in perimenopause or menopause by 2030, insurers and health systems are beginning to integrate menopause-specific care pathways.
Tools offering cognitive-support modules, cardiovascular risk tracking, and metabolic change monitoring will likely become standard, especially those like Elektra Health combining telemedicine care with evidence-based education.
5. The consumer–clinician bridge will narrow
Women increasingly expect their digital tools to generate data they can share with providers.
In 2026, more apps will automatically produce structured summaries for clinicians, covering pain patterns, autonomic signals, cycle changes like Mira Fertility, or medication effects.
Early pilots are underway exploring integration of pelvic sensor data into PT workflows and autonomic summaries into functional medicine assessments.
About the Author
Celine Vignal is the co-founder of Seesaw Health focused on female physiology, stress regulation, and preventive care.
Her work centers on translating complex nervous-system science into accessible tools and biofeedback parasympathetic breathwork methods that support everyday resilience and nervous system balance.













By Dr Fran Conti-Ramsden, clinician at Guy’s and St Thomas’ NHS Foundation Trust, academic at King’s College London, and chief medical officer of MEGI Health.
A woman gives birth. A few days later she goes home, often with a bag of medication for her blood pressure, and then, very often, very little structured follow-up for her heart (cardiovascular) health.
In my clinical work, and through our collaboration with Action on Pre-eclampsia, I see and hear about this postnatal cliff edge again and again, and it still shocks me.
We invest a lot of medical care and attention whilst a woman or birthing individual is pregnant, then, at the very moment emerging evidence suggests we have a window of opportunity to modify long-term health, the support falls away.
That cliff edge is a symptom of a deeper issue: we have come to treat “women’s health” as a synonym for reproductive health. Pregnancy, periods and fertility, important as they are, have crowded out everything else.
Yet the conditions that do most to shorten and limit women’s lives are not reproductive at all.
Cardiovascular disease is the leading cause of death in women worldwide, and it is still too readily thought of as a man’s problem.
Heart disease in women is more likely to be missed and under-treated, in part because for decades women were under-represented in the research that built our knowledge.
Pregnancy makes this vivid.
Conditions such as pre-eclampsia are not only risks to be managed for nine months; they are early warnings about a woman’s future, markers that she is more likely to develop heart disease and high blood pressure in the years to come.
We have the knowledge to act on that. What we mostly do instead is discharge her and look away.
This is exactly the kind of problem better tools should help us solve: spotting risk earlier, supporting women and their clinicians through the vulnerable postnatal window, and providing continuity where the system currently provides a drop due to lack of capacity.
Artificial intelligence and digital health have real potential here; in risk prediction, in monitoring blood pressure at home, and in helping stretched clinicians know who needs attention and when.
And yet this is not where most of the energy is going.
It is far easier to build, fund and scale an app that tracks a cycle than a tool that changes the trajectory of a woman’s heart.
So, innovation clusters at the lighter, lower-risk end of innovation, while the conditions that actually kill and disable women, and moments like the postnatal cliff, stay under-served.
Closing the women’s health gap could add at least a trillion dollars to the global economy each year, the World Economic Forum estimates, but the bigger prize is women living longer, healthier lives.
None of this means technology is a cure in itself. It is a tool, and a tool built carelessly can do harm.
Because women have been under-represented in medical data, systems trained on that data can quietly carry the same blind spots forward, deepening inequalities rather than closing them.
Responsible innovation, with clinical-grade evidence, privacy and equity designed in from the start, and tools built around real clinical pathways rather than bolted on afterwards, is not a brake on progress.
It is the only version of progress worth having.
I am optimistic, because a serious community is forming around exactly these questions and the appetite to get it right is real.
It is why, at MEGI, we are bringing clinicians, researchers, founders, regulators and investors together for our AI × Women’s Health summit on 25 June.
If we keep our focus on the conditions that matter most to women’s lives, and build the tools to meet them responsibly, the postnatal cliff edge could become something else entirely: the moment the system finally catches her and delivers preventative healthcare.
AI × Women’s Health: Innovation, Challenges and Opportunities summit is taking place on Thursday 25 June 2026 at the London Institute for Healthcare Engineering. The event is free and is fully booked and operating a waiting list. Join the waiting list here.
About Dr Fran Conti-Ramsden
Dr Fran Conti-Ramsden is a UK Obstetrics and Gynaecology registrar and Chadburn Clinical Lecturer at KCL passionate about transforming women’s health through technology and innovation.
Combining NHS clinical experience with an MRC-funded PhD, recent NHS Clinical AI fellowship and commercial role as Chief Medical Officer at Megi health, she works at the intersection of clinical medicine, data science, technology and AI.
Her current programme of research focuses on the intersection of healthcare and technology; leveraging advances such as smartphone based vital signs capture and large language models to drive forward scalable innovation in maternal cardiovascular care.
She has published over 20 peer-reviewed manuscripts (See gScholar, h-index 12), including award-winning work recognized by Hypertension Journal.
She was awarded an AI visionary award in 2025 by Health Innovation KSS was the recipient of the 2024 International Society for the Study of Hypertension in Pregnancy Zuspan prize.


By Women As One
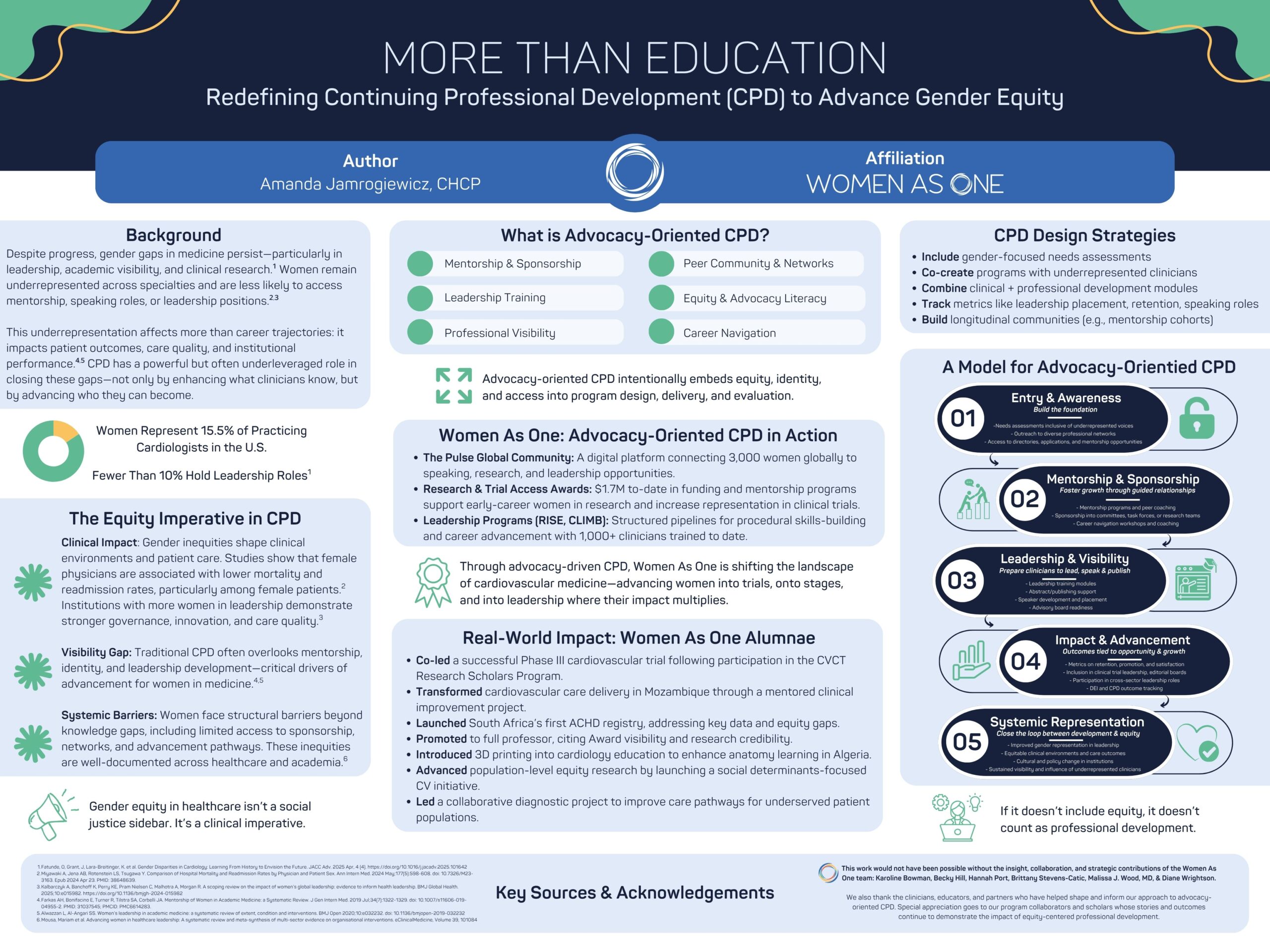
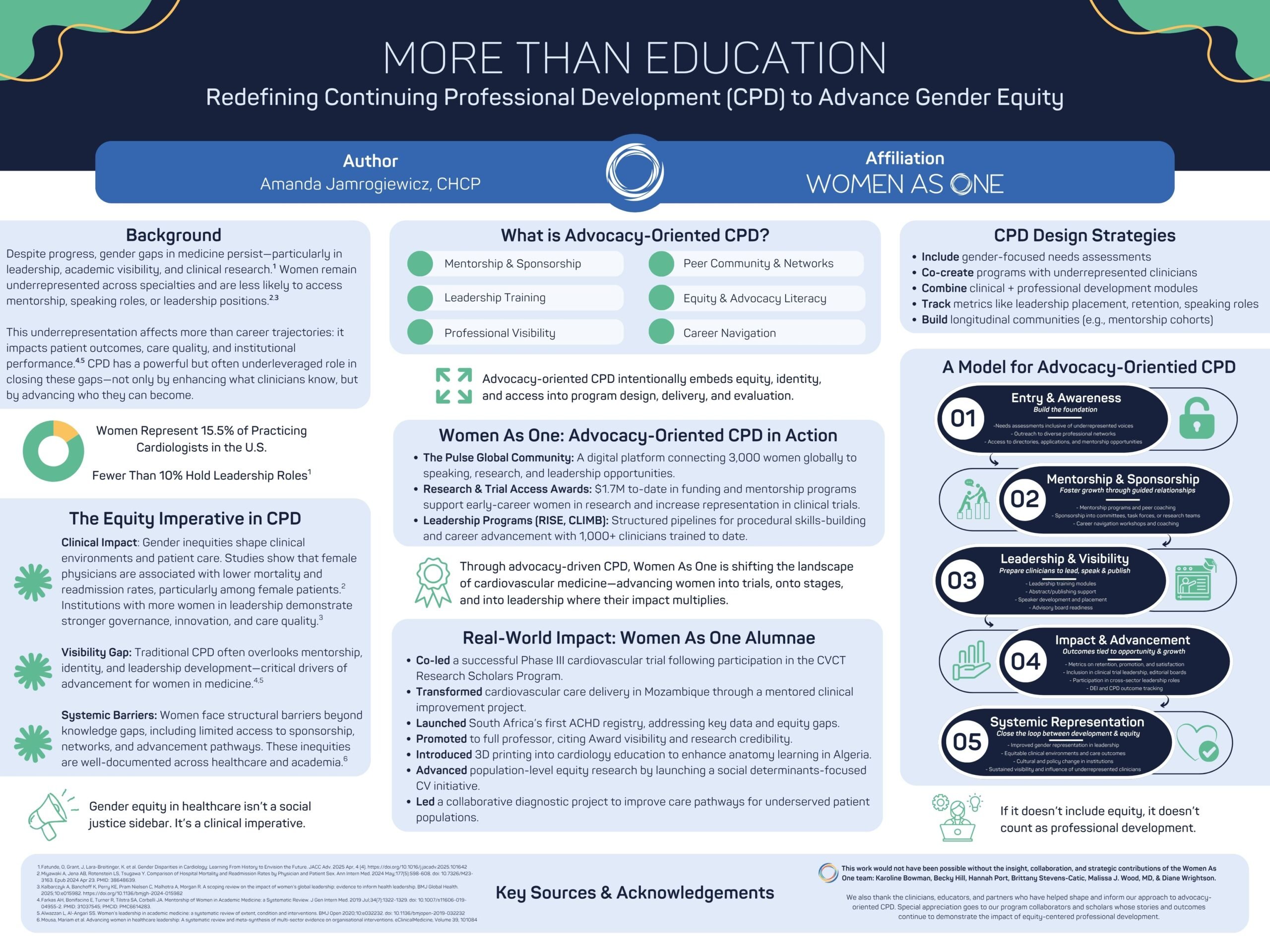
At the 2026 Alliance Annual Conference, Women As One presented a poster that asked a powerful question: What if continuing professional development (CPD) did more than teach clinical knowledge— and instead helped shape the future of the workforce itself?
For decades, professional education in medicine has focused primarily on what clinicians know and how they practice. That work remains essential.
But persistent gender gaps across cardiology—from leadership positions to research participation and speaking opportunities—demonstrate that knowledge alone is not enough to ensure equitable advancement.
To truly strengthen the field of cardiology, professional development must also support who clinicians become, the opportunities they access, and the voices that shape the future of cardiovascular medicine.
Our poster, More Than Education: Elevating Equity and Identity Through CPD, explores how a new model of advocacy-orientated CPD can help close these gaps.
Advocacy-orientated CPD expands the traditional model of professional education. In addition to building clinical expertise, it intentionally supports the structural elements that shape career advancement—mentorship, sponsorship, leadership development, visibility, and professional networks.
By integrating these elements into professional education, CPD can become a powerful engine for advancing equity—and ultimately improving patient care.
Why this matters
Gender inequities in medicine are not simply workforce issues. They influence research priorities, clinical trial representation, leadership decision-making, and ultimately the care patients receive.
When women clinicians have equitable opportunities to lead, research, and shape clinical practice, the entire healthcare system benefits.
Yet structural barriers remain. Women physicians often have less access to mentorship, sponsorship networks, and leadership pathways—factors that are critical for career advancement.
This is where advocacy-orientated CPD comes in.
By intentionally designing programs that foster mentorship, build leadership skills, create visibility, and support long-term professional growth, organizations can help ensure that the next generation of cardiovascular leaders reflects the diversity of the patients they serve.
Turning opportunity into impact
Since its founding, Women As One has supported thousands of women cardiologists across more than 100 countries, expanding access to mentorship, research opportunities, and leadership development.
Through programs like CLIMB, RISE, Mentorship Awards, and our global digital community, The Pulse, thousands of women cardiologists have gained mentorship, leadership training, and opportunities that accelerate their careers and expand their influence.
Today, the outcomes of these programs are shaping the field in tangible ways:
- Women As One alumnae are leading clinical trials and advancing cardiovascular research
- Clinicians supported through our programs are building registries, launching new care models, and expanding access to specialized care
- Women cardiologists are gaining greater representation on speaker panels, advisory boards, and leadership pathways
- A global community of more than 3,000 women cardiologists is strengthening collaboration, mentorship, and visibility across the profession
These outcomes demonstrate what becomes possible when professional development goes beyond traditional education to intentionally support leadership, identity, and community.
A call to the cardiovascular community
Advancing equity in cardiology is not the responsibility of one organization—it requires a collective effort across the entire ecosystem of clinicians, educators, institutions, and industry partners.
For women cardiologists, this means engaging in the programs, mentorship networks, and leadership opportunities that help shape the future of the field. Whether through CLIMB, RISE, research initiatives, or participation in The Pulse community, your involvement strengthens a growing movement dedicated to advancing women in cardiology.
For our partners and supporters, this work demonstrates the powerful impact that strategic investment in equity-focused professional development can have on the workforce and the patients we ultimately serve.
Together, we can redefine what professional development looks like in medicine—not just as a pathway for learning, but as a catalyst for leadership, opportunity, and lasting change.
Explore the poster
We invite you to explore the poster below (click here to download it) to learn more about the evidence, framework, and real-world impact behind this work—and to join us in continuing to expand what professional development can achieve for the future of cardiovascular medicine.
Learn more about Women As One at womenasone.org
Opinion
What Maternal Mental Health Month reveals about where postpartum support actually breaks down

By Morgan Rose, chief science officer at Ema, and Lauren Scocozza, vice president of product at Willow
May is Maternal Mental Health Month, and every year it surfaces a familiar set of statistics: 1 in 5 new mothers experiences postpartum depression or anxiety, most go unscreened, and the majority who are screened don’t receive adequate follow-up care.
The conversation is important. But the numbers obscure something that anyone who has worked in this space knows to be true: postpartum mental health distress rarely arrives with a label.
It arrives as exhaustion. As “I’m not sure I’m doing this right.”
As a question about supply, pumping, whether it’s okay to feel this disconnected from something you were supposed to love immediately.
Willow integrated Ema, AI built for women’s health, with the goal of closing the maternal care and data gap.
The pattern mentioned above appears consistently in Ema’s conversational data through the Willow app.
A mother reports mastitis symptoms.
Ema walks her through the clinical presentation, confirms she should keep pumping, and then she questions if she is using her pump correctly. In the same thread, within a few exchanges, she says she’s “feeling too sad.” Then: “I don’t know. I think I’m depressed. I am not enjoying my postpartum.”
She did not come to the app to talk about her mental health.
She came about a breast infection. The mental health disclosure came through the already-opened door.
The Weight Underneath the Technical Question
New motherhood involves an enormous amount of problem-solving at a time when cognitive and emotional reserves are depleted. The pump has to work. The baby has to eat. The body has to recover.
Work comes back. Sleep doesn’t. Feeding their babies requires skill, and the learning curve sits atop it all.
What Ema’s conversation data shows is that the emotional load of navigating these challenges is not separate from mental health. It is mental health.
When a mother writes, “I’m postpartum and overwhelmed and tired,” and then, in the same breath, asks about flange sizing, she is telling us what the postpartum experience actually feels like from the inside.
The technical question and the emotional state are one and the same.
Breastfeeding carries particular weight here.
The desire to breastfeed, the guilt when it doesn’t go as planned, and the identity questions that come with feeding choices are not peripheral to the postpartum mental health conversation.
In our conversations, women navigating supply concerns often reveal deeper anxieties: about whether they are good mothers, whether their bodies are “working,” and whether the difficulty they are experiencing means something about them.
These are the signals worth asking about.
What Screening Looks Like in Practice
Ema is trained on the Edinburgh Postnatal Depression Scale and is equipped to offer the EPDS when a conversation warrants it.
The value is being present for the moment when a woman is ready to name what she’s feeling.
That moment rarely comes as a direct request for mental health support. It comes when someone is already in a conversation about something else, and something shifts.
A woman dealing with mastitis says she feels sad. A woman worried about supply says she doesn’t feel like herself. A woman managing the logistics of going back to work with a wearable pump says she’s not sure she can keep up with it all — and the “it all” isn’t about the pump.
Ema is designed to hear that. She doesn’t stay on the clinical or technical track when the conversation moves. She follows the person.
And when the moment is right, she offers the screening as a natural next step.
In one exchange, a woman was offered the EPDS after disclosing depressive feelings. She declined.
Ema acknowledged that and asked if she wanted to talk about something else. That’s the right response. The offer was made without pressure. The door stays open.
Sometimes what matters most is that someone asked at all.
The Continuity Problem
One of the most persistent structural failures in maternal mental health care is fragmentation.
A woman sees her OB at six weeks postpartum for a brief screening. She may get a call from a nurse. She may be given a referral she never follows up on because she doesn’t have the capacity to navigate a new care relationship while managing a newborn.
The clinical touchpoints are too few, too far apart, and too often siloed from one another.
The postpartum period lasts far longer than the six-week checkup implies. Mental health symptoms can emerge weeks or months after delivery, shift in character over time, and interact with physical challenges in ways that don’t fit neatly into any single provider’s lane.
A lactation concern becomes an anxiety spiral. A supply drop triggers a grief response. A difficult return to work surfaces a postpartum depression that wasn’t fully recognized at six weeks.
Ema sits inside these moments because she’s embedded in the platform women are already using. She doesn’t require a separate appointment, a referral, or the cognitive bandwidth to seek out a new resource.
She’s in the Willow app that mom is already using multiple times a day to manage her pump.
When Ema identifies a woman who may need more support than she can provide, she routes to the right resource — whether that’s a SimpliFed lactation consultant for feeding-related concerns or a clinical professional for mental health follow-up.
The conversation leads to the handoff with someone who can do more.
What the Month of May Means for the Rest of the Year
Maternal Mental Health Month is a useful moment of attention. The awareness campaigns, the social media posts, and the statistics shared in newsletters matter.
But the gap in postpartum mental health care is not really an awareness problem.
Most people in the perinatal space and beyond know the statistics. The problem is access, timing, and continuity.
AI doesn’t close that gap on its own.
What it can do is be present in the spaces where women already are, at the times when they need something, and attentive enough to recognise that a conversation about a pump, a clogged duct, or a supply concern is also a conversation about how someone is doing.
The question behind the question is often the more important one.
For Willow, the conversation data Ema generates is a map of where mothers are struggling, what they reach for when they need help, and when they are ready to say more than they came to say.
That information, used well, shapes better resources, better onboarding, and a more connected experience across the full arc of the postpartum year and beyond.
Building the infrastructure to support maternal mental health is a year-round project.
Willow is doing one part of that, and the conversations happening on the Willow platform every day are evidence that women want support that meets them where they are… in their app, in their moment, without having to ask for it twice.
About the authors
Morgan Rose is Chief Science Officer at Ema, an AI platform for women’s health. Ema partners with healthcare organisations and femtech companies to deliver clinically grounded AI support across the perinatal journey.
Lauren Scocozza is the Vice President of Product at Willow Innovations, Inc. For women by women, Willow is building a maternal care platform to address the interconnected challenges of postpartum.










{kind=link}

 Menopause4 weeks ago
Menopause4 weeks agoPerimenopause misinformation ‘putting women at risk’

 Entrepreneur4 weeks ago
Entrepreneur4 weeks agoWomen’s Health Innovation Summit opens submissions for 2026 Innovation Showcase

 Insight3 weeks ago
Insight3 weeks agoBritish women among angriest in Europe, health survey reveals

 Menopause4 weeks ago
Menopause4 weeks agoWomen still being failed when they reach menopause, experts say

 Menopause4 weeks ago
Menopause4 weeks agoSweden eyes domestic production of oestrogen patches amid menopause treatment shortage

 Menopause2 weeks ago
Menopause2 weeks agoApple Health adds menopause and perimenopause tracking

 News2 weeks ago
News2 weeks agoFemtech World Awards 2026: Winners revealed

 News4 weeks ago
News4 weeks agoThree menopause innovators shortlisted for Femtech World Award