




Entrepreneur
Interview: Closing the gap in care for high-risk pregnancies

Pregnolia is on a mission to transform pregnancy care by bringing an often-overlooked biomarker into clinical practice. Stephanie Price speaks to founder and CEO Dr. Sabrina Badir to find out more.
Paying closer clinical attention to cervical stiffness could hold the key to better outcomes for high-risk pregnancies.
That is according to Pregnolia, a Swiss university spin-out founded in 2016, which is working to improve pregnancy care through the detection of cervical changes that contribute to the risk of preterm birth.

Its technology measures the stiffness of the cervix to aid pregnancy management, providing quantitative data to support clinical decisions quickly.
The company emerged out of research at ETH Zürich university and the University Hospital in Zürich into changes in cervical stiffness during pregnancy.
“During our research, we identified cervical stiffness as a critical yet overlooked biomarker in pregnancy,” says Pregnolia founder and CEO, Dr. Sabrina Badir.
“This insight became the foundation for the Pregnolia system – a CE-marked and patented medical device that enables objective and precise measurement of cervical stiffness.
Badir says that one in 10 babies are born too early, resulting in consequences such as higher risk of death, underdeveloped lungs, neurological impairment and chronic illness – causing high costs for families and healthcare systems.
Driven by a mission to improve prenatal care and tackle some of the most pressing unmet needs in obstetrics, Badir explains that Pregnolia’s goal is to detect changes in cervical stiffness earlier and accurately measure the changes.
According to Badir, the Pregnolia system outperforms traditional methods, which focus on evaluating cervical length and dilation using ultrasound techniques, and reduces the risks associated with preterm births, as well as assessing cervical readiness for labour induction.
“With this platform technology, we support clinicians in making earlier and better-informed decisions in pregnancy care, ultimately improving outcomes for mothers and babies worldwide.
“Our long-term vision is clear: to bring cervical stiffness into clinical routine – not only to improve care for high-risk pregnancies, but ultimately to enable universal screening and make pregnancy monitoring more precise, proactive, and equitable.”
As the world’s first CE-marked and patented medical device for measuring cervical stiffness, Badir explains that the system consists of two components including a reusable control unit and a sterile, single-use probe.
“The system uses a gentle aspiration technique,” says Badir. “When the probe is placed on the cervix, it gradually applies a controlled vacuum that gently lifts the tissue.
“Once the cervix lifts by four millimetres, the system records the pressure needed to reach that elevation. The stiffer the tissue, the more pressure is required. This value is shown immediately as the Cervical Stiffness Index (CSI).
“The Pregnolia system provides a fast, easy-to-use, and objective measurement. Cervical stiffness has shown promising diagnostic performance, even outperforming cervical length measurement by ultrasound in certain clinical situations.
“The technology is scalable and suitable for use in both high-resource and low-resource settings.”
Badir explains that Pregnolia is now working with OBGYN experts to integrate cervical stiffness assessment into clinical practice by developing digital companion tools, expanding clinical validation, and preparing for inclusion in national guidelines and reimbursement frameworks.
The Pregnolia system originated from Badir’s doctoral research at ETH Zurich in collaboration with the University Hospital Zürich which led to the development of a new method to quantify cervical stiffness.
“This interdisciplinary environment – where engineering met obstetrics – was the perfect setting for innovation.
“Together with clinicians, we identified the lack of objective tools to assess cervical readiness as a major limitation in prenatal care.
“I’m proud that what began as an academic idea is now a certified medical device with the potential to redefine standards of care in obstetrics.
“We’re also proud to have secured over [USD$3.77m] in non-dilutive funding to support our development efforts. In 2019, Pregnolia was awarded a prestigious €1.5m grant from the European Union under the Horizon 2020 SME Instrument, which is now part of the EIC Accelerator programme.
“This support enabled us to scale up production and prepare the Pregnolia system for market introduction in Europe.
“Beyond the financial contribution, the EU’s backing was also a strong endorsement of the impact and innovation behind our technology, and it played a key role in helping us raise over [USD$12.58m] in equity funding to date.”
With preterm birth being one of the leading challenges for maternal health and newborn health, Pregnolia is working to support the unmet need for sufficient risk measuring tools.
Badir says that despite decades of research and various public health initiatives, current tools for assessing the risk of preterm birth remain insufficient.
“Ultrasound-based cervical length, digital exams, and biochemical markers often lack sensitivity and reproducibility,” says Badir.
“Many at-risk women go undetected, while others receive unnecessary treatment due to false positives.
“The Pregnolia system addresses this gap by providing an objective, point-of-care measurement of cervical stiffness, a new biomarker for the risk of preterm birth.”

The Pregnolia system supports clinical decision-making in both symptomatic women, helping triage patients more precisely and avoiding overtreatment, and in asymptomatic high-risk women, helping to detect mothers that may benefit from early interventions.
“In the future, cervical stiffness could also become an important parameter for guiding induction of labor, which is becoming increasingly common and complex,” says Badir.
“By improving risk stratification and supporting clinical decisions, Pregnolia has the potential to reduce unnecessary interventions, allocate resources more efficiently, and improve outcomes, especially in health systems with limited capacity.”
Pregnolia was the winner of the Femtech World OBGYN Innovation of the Year Award 2025, sponsored by elitone by Elidah.
The award, says Badir, recognises not the technology and the collective effort behind it.
“It energises us for the next phase of our journey. Pregnolia is CE-marked and ready for market entry in Europe. But through our collaborations, especially with clinical leaders in the UK, we’ve learned that the value of our innovation can be expanded even further.”
Badir explains that Pregnolia is now investing in additional clinical studies to support broader adoption, reimbursement, and integration into clinical routines.
“At the same time, our business development efforts are focused on identifying the right strategic partner, ideally one with established commercial operations, who can help maximise the value and reach of Pregnolia.”
This year, the company will also be advancing new clinical indications based on cervical stiffness, progressing its US regulatory strategy, including FDA discussions and raising further funds.
“Bringing a new diagnostic technology into clinical practice is never a solo effort. At Pregnolia, one of our greatest strengths is the global network we’ve built,” says Badir.
“This collaborative ecosystem has been instrumental in advancing our clinical research, generating the evidence needed to build trust, shaping regulatory strategies, and exploring adoption pathways in diverse healthcare settings.
“But it’s also a reflection of how we work: we listen, we learn, and we co-develop with those closest to patient care.
“We believe this network-driven approach is not only key to Pregnolia’s success, but a model for how innovation in obstetrics can and should evolve: rooted in science, focused on clinical impact, and built through global collaboration.”












Juno Bio has secured US$3.8m to expand its diagnostics platform for vaginal health and reproductive care.
The funding round was led by Ada Ventures, with participation from Artesian, Entrepreneur First and Illumina Accelerator.
The women’s health startup said the seed funding will support the launch of its first CLIA-certified sequencing laboratory in Oakland, California, and a new clinical vaginal microbiome and STI test for healthcare providers.
CLIA certification refers to US laboratory standards for testing human samples used in diagnosis, prevention or treatment decisions.

Dr Leighton Turner, co-founder and chief scientific officer of Juno Bio, said: “The vaginal microbiome is still one of the least understood systems in the body at a clinical scale.
“With our lab, we’re starting to build a measurement standard that clinicians can actually use.
“We believe the level of detail from this kind of testing can meaningfully improve how vaginal healthcare is provided.”
The company is developing precision diagnostics for vaginal health, where patients can experience recurring symptoms, inconsistent diagnoses and treatments based on trial and error.
Juno Bio said bringing testing in-house gives it greater control over the process, from sample handling to results, while allowing it to refine its technology and build what it says is one of the largest datasets focused on the vaginal microbiome.
The vaginal microbiome is the community of bacteria and fungi that naturally live in the vagina. Changes in this balance can be linked to infections, symptoms and wider reproductive health issues.
Juno Bio’s newly launched clinical test examines the wider vaginal microbiome and screens for four common sexually transmitted infections, or STIs.
Rather than looking for a single cause, the test is intended to give clinicians a broader picture of what may be contributing to symptoms.
Juno Bio says this matters because multiple infections can occur at the same time and microbiome changes may be linked to fertility, menopause or recurrent infections.
Dr Anna Powell of Johns Hopkins said: “Vaginal microbiome testing has the potential to significantly reshape how we understand and manage vaginal health, particularly for patients with recurrent or unexplained symptoms.
“While the field is still evolving, advances in sequencing and data interpretation are moving us closer to a future where more personalised, microbiome-informed care can complement existing diagnostic approaches.”
Check Warner, co-founding partner at Ada Ventures, added: “Juno Bio is setting a new standard for how vaginal health is understood and managed.
“What they’ve built at this stage, with this level of capital efficiency, is exceptional.
“We’re proud to support the team as they scale their clinical infrastructure and continue leading innovation in this critically underserved category.”

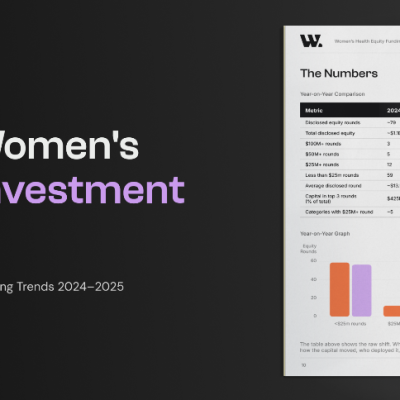
Women’s health companies raised a record $1.55 billion in disclosed equity in 2025, up 41 per cent year on year, according to W Group’s first Global Women’s Health Investment Report, The Road to the Era of Scale.
The report tracks over 500 funding stories and 164 equity rounds across 15 categories and 30+ countries.
Eighty-five companies raised equity in 2025, the highest single-year count on record. But according to the report, the headline figure isn’t the most significant one.
The bigger shift is in where that capital went and how concentrated it was at the top compared to the year before.
The report also points to a brand new investment category that didn’t exist twelve months ago.
SheMed closed a $50 million Series A this year to build a women-specific GLP-1 and metabolic health platform, the first dedicated raise of its kind.
Alongside the momentum, the report identifies one structural risk that could determine whether 2025’s growth holds: a bottleneck at Series A that’s leaving a number of promising seed-stage companies stuck.
Molly Taylor, head of content at W Group, said: “2025 was the biggest year women’s health has ever had, and the most important finding isn’t the headline number.
“It’s that the money has stopped pooling at the top.
“Capital is reaching more companies, more categories and more countries than ever before. The Era of Scale is real. It’s just not finished, and the Series A gap is where it could stall.
“Closing that gap is the highest-leverage move this ecosystem can make in 2026.”
Read the full report: https://wplatform.co/forms/womens-health-equity-funding-trends-report-2026?utm_source=advocacy&utm_medium=ext_email&utm_campaign=2026-q3-health-report-femtech-world
Onto Health has acquired Levy Health, a fertility software company providing precision diagnostics and patient intake for reproductive medicine.
The acquisition, fuelled by Onto Health’s US$20m Series A fundraise in April, supports its plan to build scalable, tech-enabled infrastructure for reproductive medicine.
Onto founder Roohi Jeelani, MD, called it the first of several moves in the company’s expansion strategy in a LinkedIn post, adding that there was “more coming soon”.

She said: “This isn’t just an acquisition, it’s proof of how we’re building Onto: physician-led, tech-enabled, and built to scale without losing the personal touch fertility patients deserve.”
Headquartered in Chicago, Onto Health combines evidence-based fertility care with artificial intelligence-driven diagnostics, clinical automation and longevity science.
AI-driven diagnostics use software to analyse patient information and support clinical decision-making, rather than replace clinicians.
Levy Health, founded in Berlin with US offices in San Francisco, helps medical providers identify endocrine disorders more quickly and helps clinics streamline fertility workups.
Endocrine disorders affect the body’s hormone system, which can influence ovulation, menstrual cycles and fertility.
Co-founder Caroline Mitterdorfer said joining Onto would expand Levy Health’s fertility care tools to more clinics and patients, helping physicians focus on patient care.
Onto opened its first clinic in Chicago in February, with plans for three more in the greater Chicago area.
The company said in April that it would use its new funding, led by Artis and Humania, to support additional operations in the US and expand into the Gulf Cooperation Council.
The Gulf Cooperation Council includes six Arab states bordering the Persian Gulf.








 Insight2 weeks ago
Insight2 weeks agoWomen with PMOS should have annual NHS checks, new guidance says

 Diagnosis1 week ago
Diagnosis1 week agoTwo “gamechanger” tests set to speed up endometriosis diagnosis on the NHS

 News3 days ago
News3 days agoNew menopause drug approved for use by NHS in Scotland

 Cancer1 week ago
Cancer1 week agoThousands of women could avoid painful cancer exam with new AI blood test

 News2 weeks ago
News2 weeks agoBreast cancer biosensor and low-cost ultrasound startups win women’s health AI competition

 Entrepreneur1 week ago
Entrepreneur1 week agoApplications open for the third W Accelerate with Merck KGaA and M Ventures

 News2 weeks ago
News2 weeks agoClue spotlights seven women’s health journeys in new campaign

 Fertility1 week ago
Fertility1 week agoOlder women face lower chance of fertility treatment working, even with donor eggs, study finds
2 Comments